Ventricular Septal Defects
Ventricular Septal Defects. Tate Gisslen, MD Mentor: Bradley S. Marino, MD, MPP, MSCE May 6, 2011. Anatomy. 4 morphological components of septum Membranous Inlet Outlet/Infundibular Muscular/Trabecular. Anatomy. Membranous-70-80% Small Located at base, between inlet and outlet

Ventricular Septal Defects
E N D
Presentation Transcript
Ventricular Septal Defects Tate Gisslen, MD Mentor: Bradley S. Marino, MD, MPP, MSCE May 6, 2011
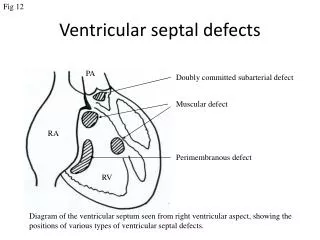
Anatomy • 4 morphological components of septum • Membranous • Inlet • Outlet/Infundibular • Muscular/Trabecular
Anatomy • Membranous-70-80% • Small • Located at base, between inlet and outlet • Perimembranous - Extends to adjacent septum Membranous Membranous
Anatomy • Inlet • Inlet 5-8%, • AV valve to chordae attachments Inlet
Anatomy • Outlet/Infundibular • 5-7% • Separates L and R outflow tracts Infundibular
Anatomy • Muscular/Trabecular (5-20%) • Anterior/Marginal (anterior to septal band) • Midmuscular/Central (posterior to septal band) • Apical (inferior to moderator band) • Posterior (beneath septal leaflet) Muscular
Physiology • Blood flow (which way and how much) dependent on multiple factors • Small and restrictive • Lesion size • Large and non-restrictive • Balance between pulmonary and systemic vascular resistance
Lesion Size • Restrictive VSD • < 0.5 cm2 (Smaller than Ao valve orifice area) • Small L to R shunt • Normal RV output • 75% spontaneously close < 2yrs • Non-restrictive VSD • > 1.0 cm2 (Equal to or greater than to Ao valve orifice area) • Equal RV and LV pressures • Large hemodynamically significant L to R shunt • Rarely close spontaneously
Vascular Resistance • Pulmonary resistance may remain high longer in infants with large VSD • Minimal L to R shunt • Decreasing pulmonary resistance leads to significant L to R shunt • Clinical symptoms of CHF • Persistent L to R shunt leads to hypertrophy of the medial smooth muscle layer of the pulmonary arteries which increases PVR and potential R to L shunting • Long-standing L to R shunting that results in chronically increased PVR may lead to persistent R to L shunting described as “Eisenmenger Physiology”
Clinical Features-Small Lesions • Murmur • 4 to 10 days, early with rapid decrease in PVR • Asymptomatic • normal feeding, growth and development
Murmurs • Restrictive VSD - Holosystolic murmur • correlates with continuous pressure gradient • Non-restrictive large VSD – no murmur (no turbulence if no gradient)
Clinical Features-Large Lesions • Accentuated precordial activity • More prominent as LV volume increases • Signs/symptoms of CHF • Diaphoresis • Tachypnea • Fatigue with feeding • Hepatomegaly • Rales • Duskiness with crying • May develop as early as 2 weeks • Severity increases as PVR decreases
Evaluation • Chest Radiography • Cardiomegaly • Increased pulmonary vasculature • Pulmonary edema
Evaluation • EKG • Small: normal or LVH • Prominent Q, R, and T waves in II, III, aVF and V6 • Large: Biventricular hypertrophy • RVH- rsR’ in V1, S wave in V6
Echocardiography • Assess indication in consultation with Cardiology • Assess location, size, and multiplicity • RV and PA pressure • Assess for LA and LV dilation • Assess LV function • Note relation to great vessels, AV valves
Cardiac Catheterization • Able to document • Number of defects • Presence of associated defects • Magnitude of shunt • Estimate PVR • Not used if information apparent by other means • Most information available through Echocardiography
Prevalence • Most common congenital heart lesion • Occurs in 50% of children with heart lesions • 15-20% in isolation • 5-50 per 1000 live births • 56% female
Associated Defects • Left Heart Defects • Aortic stenosis • Coarctation of the aorta • Right Heart Defects • Tetrology of Fallot • Double Outlet Right Ventricle • Truncus Arteriosus • Some single ventricle (e.g. Tricuspid atresia, double inlet left ventricle)
Chromosomal Disorders associated with VSD • Trisomy 21: 40% of T21 will have VSD • Trisomy 13, 18: 18% of T13, 31% of T18 will have VSD • 22q11 deletion: • Tetrology of Fallot is most common anomaly • VSD with or without aortic arch anomaly is second most common • Holt-Oram (Hand-heart syndrome): TBX5 gene found on Chromosome 12 • Recurrence risk for VSD based on parental VSD • Paternal 2% • Maternal 6-10%
Treatment for Small VSD • No medication or surgery if asymptomatic • 75-80% close by 2 years • Observation • No antibiotic prophylaxis for procedures
Treating a Moderate to Large VSD • Treatment of CHF • Determining when to repair
CHF Treatment • High-calorie formula • Medication • Diuretics • Furosemide with or without spironolactone • Afterload reduction • Enalapril or Captopril • Digoxin (maybe) • Symptoms of CHF improve as L to R shunt decreases
Indications for Intervention • Decompensated CHF • Compensated CHF with: • Large hemodynamically significant VSD - L to R shunting with Qp/Qs > 2:1, even if asymptomatic, ideally before 1 year • Growth failure, unresponsive to medical therapy is an indication for surgery
Not Indicated • Small VSDs - 6 months without CHF or ↑PVR • Small hemodynamically insignificant VSD – L to R shunting with Qp/Qs < 1.5:1 • Eisenmenger physiology
Post-Intervention • Most infants have normal growth and development • Early closure (< 1 year) associated with better LV function and regression of hypertrophy • Residual VSD is not common • RBBB is common following surgery • Rare complete heart block
Surgery • Typically dacron patch closure • Sometimes primary closure • Surgical mortality < 1%
Catheter Closure • Location • Muscular • Perimembranous • Complications • Heart block • Valve insufficiency
References • Backer CL. Ventricular septal defect closure: what is the role for transcatheter closure? Cardiology. 2009;114:235-7. Epub 2009 Aug 7. • Beck AE, Hudgins, L. Congenital cardiac lesions in the neonate: Isolated or syndromic? Neoreviews. 2003;4:e105-e110. • Carminati M, Butera G, Chessa M, De Giovanni J, Fisher G, Gewillig M, Peuster M, Piechaud JF, Santoro G, Sievert H, Spadoni I, Walsh K; Investigators of the European VSD Registry. Transcatheter closure of congenital ventricular septal defects: results of the European Registry. Eur Heart J. 2007;28:2361-8. Epub 2007 Aug 7. • Knauth AL, Lock JE, Perry SB, McElhinney DB, Gauvreau K, Landzberg MJ, Rome JJ, Hellenbrand WE, Ruiz CE, Jenkins KJ. Transcatheter device closure of congenital and postoperative residual ventricular septal defects. Circulation. 2004;110:501-7. Epub 2004 Jul 19. • Maghsood S, Das BB. Index of suspicion in the nursery. Neoreviews. 2007;8:e133-e135 • McDaniel NL, Gutgesell HP. Ventricular septal defects. In: Allen HD, Clark EB, Gutgesell HP, Driscoll DJ, eds. Moss and Adams’ Heart disease in infants, children and adolescents. Philadelphia: Lippincott Williams & Wilkins, 2001:636-651. • Minette MS, Sahn DJ. Ventricular septal defects. Circulation. 2006;114:2190-2197. • Momma K, Matsuoka R, Takao A. Aortic arch anomalies associated with chromosome 22q11 deletion (CATCH 22). Pediatr Cardiol. 1999;20:97-102. • Park MK. Pediatric Cardiology for Practitioners. St. Louis: Mosby, Inc. 1996:135-142. • Park MK. The Pedatric Cardiology Handbook. Philadelphia: Mosby Elsevier, 2003:67-70. • Pont SJ, Robbins JM, Bird TM, Gibson JB, Cleves MA, Tilford JM, Aitken ME. Congenital malformations among liveborn infants with trisomies 18 and 13. Am J Med Genet A. 2006;140:1749-56. • Wilson W, Taubert KA, Gewitz M, Lockhart PB, Baddour LM, Levison M, Bolger A, Cabell CH, Takahashi M, Baltimore RS, Newburger JW, Strom BL, Tani LY, Gerber M, Bonow RO, Pallasch T, Shulman ST, Rowley AH, Burns JC, Ferrieri P, Gardner T, Goff D, Durack DT; American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee; American Heart Association Council on Cardiovascular Disease in the Young; American Heart Association Council on Clinical Cardiology; American Heart Association Council on Cardiovascular Surgery and Anesthesia; Quality of Care and Outcomes Research Interdisciplinary Working Group. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation. 2007;116:1736-54. Epub 2007 Apr 19. • Zahka KG, Gruenstein DH. Approach to the neonate with cardiovascular disease. In: Martin RJ, Fanaroff AA, Walsh MC, eds. Neonatal-Perinatal Medicine. Philadelphia: Mosby Elsevier, 2006:1747-1754.