Ventricular Septal Defect
Ventricular Septal Defect. Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery. Primary Ventricular Septal Defect. 1. Definition A hole or multiple holes in the interventricular septum. A VSD may be part of another major cardiovascular


Ventricular Septal Defect
E N D
Presentation Transcript
Ventricular Septal Defect Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery
Primary Ventricular Septal Defect • 1. Definition • A hole or multiple holes in the interventricular septum. • A VSD may be part of another major cardiovascular • anomaly and may be acquired, and primary VSD may have • minor coexisting morphologic abnormalities • 2. History • Roger : 1st description in 1879 • Eisenmenger : Autopsy finding in 1897 • Lillehei, Varco : Repair using controlled cross • circulation in 1954 • DuShane et al in Mayo Clinic : Intracardiac repair • with pump oxygenator in 1955~1956 • Lillehei : Atrial approach to VSD in 1957
Ventricular Septal Defect • 1. Embryology • VSD occurs at 1st. 8 weeks of fetal life through interaction • between interventricular muscular partition, endocardial • cushions, and bulbar ridges that separate great vessels. • 2. Etiology • Chromosomal • Familial • Geographic • Environmental
Ventricular Septal Defect • Pathophysiology • Defect in the interventricular septum permits left-to-right shunting of blood • RV volume overload & pulmonary overcirculation can produce congestive heart failure in infancy & irreversible pulmonary hypertension later in life • Shunt reversal (right-to-left) due to elevated pulmonary vascular resistances leads to systemic hypoxemia (Eisenmenger syndrome)
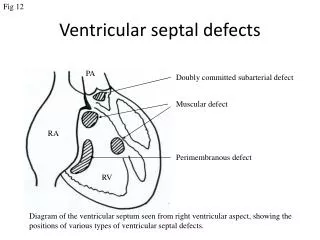
Morphology of VSD • 1. Size • 1) Large : approximately the size of aortic orifice • 2) Moderate : still restrictive, but sufficient size to raise • RV pressure to ½ ofLV and Qp/Os>2.0 • 3) Small : insufficient size to raise RV pressure & • Qp/Qs < 1.75 • 2. Location • 1) Perimembranous VSD : 80% • 2) VSD in RV outlet : 5-10% • 3) Inlet septal VSD : 5% • 4) Muscular VSD : 5% • 5) Confluent VSD • 6) VSD with straddling or overriding TV
Morphologic Classification of VSD Classification Extension Perimembranous Inlet (junctional)Anterior Outlet Muscular Outlet (conal) Trabecular Inlet Anterior Apical Doubly committed subarterial (RV outlet) Inlet septal Atrioventricular septal type Malalignment Anterior (TOF) Posterior (COA, IAA) Rotational (Taussig-Bing)
Associated Lesions with VSD • 1. PDA • 6% of all ages, 25% of infants in heart failure • 2. COA ; 5% • 3. Congenital aortic stenosis • 2% requiring operation for VSD (sub AS> valv AS) • 4. Infundibular pulmonary stenosis • 5. Congenital mitral valve disease ; 2% • 6. Absent pulmonary arteries, peripheral PS • 7. Positional anomalies
Pulmonary Vascular Disease • Grade I : Medial hypertrophy without intimal proliferation. • II : Medial hypertrophy with cellular intimal reaction. • III: Intimal fibrosis, as well as medial hypertrophy, • early vascular dilation. • IV: Generalized vascular dilation, areas of vascular • occlusion by intimal fibrosis & plexiform lesion. • V : Other dilation lesion such as cavernous and • angiomatoid lesions. • VI : Necrotizig arteritis in addition to grade V changes
Clinical Features & Diagnosis • 1. Prevalence • 2 per 1,000 live births • 20% of CHD • Associated & isolated VSD : 50% of CHD • Higher incidence in premature • 2. Clinical features • Symptoms and signs of heart failure • Cardiomegaly & large pulmonary blood flow • Pansystolic or systolic murmur • Biventricular or left ventricular hypertrophy • 3. Two-dimensional echocardiography • 4. Cardiac catheterization & angiocardiography
Natural History of VSD • 1. Spontaneous closure • 2. Pulmonary vascular disease • 3. Bacterial endocarditis ; rarely recently • 4. Premature death • 5. Clinical course • 6. Development of aortic incompetence • 7. Development of infundibular PS
Spontaneous Closure of VSD • 1. Mechanism of narrowing or closure • 1) Adherence of TV leaflet or chordae tissue • 2) Aneurysm of membranous septum erroneously related • --rarein conoventricular, juxtaarterial, AV canal, • muscular defect • 2. Rate • About 80% of VSD at 1 month eventually narrow or close • About 60% of VSD at 3 months eventually narrow or close • About 50% of VSD at 6 months eventually narrow or close • About 25% of VSD at 12 months eventually narrow or close • Becomes rare after 12 ~ 18 months of age
VSD Spontaneous Closure Probability
Pulmonary Vascular Resistance Resistance Description < unit/BSA < < 4 Normal 4 ~ 5 Mild elevated 5 ~ 8 Moderately elevated 8 > Severely elevated
PA Banding in VSD of PVD ? • This increases right-left shunt, the saturation in the aorta will fall, and so does the venous blood returning to the RA (maximally desaturated). • For the lungs, shock means low oxygen and pressure in the PA and shock is the most potent vasodilator in the body, mainly in the PA. • To reverse completely lung lesions "extracting oxygen from the PA . Once you extract it, the lung lesions reverse completely • What causes hyperresistant PA hypertension is the quantity of oxygen in the PA. If the PA would have had hyperflow with low oxygen, it would not have developed hyperresistant pulmonary hypertension
Indications for Operation • 1. Severe and intractable heart failure or respiratory • symptoms during the 1st 3months of life. • 2. Severe symptoms, growth failure, rising PVR • older than 3 months of age. • 3. VSD with PVR more than 4 unit during 6-12 months. • 4. VSD with elevated PVR first seen after infancy. • 5. Moderate VSD with no size change in childhood. • 6. Juxtaarterial , juxtaaortic VSD is a special situation.
Techniques of Operation • 1. Route • 1) Right atrium • 2) Right ventricle, or left ventricle • 3) Pulmonary artery • 2. Repair of VSD • 1) Conoventricular VSD • 2) Juxtaarterial VSD • 3) Inlet VSD • 4) Muscular VSD • 3. Closure of associated PDA • 4. Pulmonary artery banding & debanding
VSD. PMOE Patch Closure • VSD closure through anterior leaflet of TVdetachment
Apical Muscular VSD Patch Closure via RVtomy (A) Trabeculations overlying the VSD are taken down. (B) Interrupted pledgetted sutures are placed full thickness at the superior margin of the defect, maintaining the pledgets on the left ventricular side (C) Closure of the VSD with a Dacron patch
Flap Valve Double Patch Closure • Flap valve double patch closure of Ventricular Septal Defects in children with Increased Pulmonary Vascular Resistance
Closure of Trabecular VSD Sandwich Technique • Sutures & patch can be passed through the other VSD or mitral valve
1. Hospital mortality 2. Modes of early death 3. Incremental risk factors for hospital death 1) Early date of op. 2) Multiple VSD 3) Associated anomalies 4. Survival Pulmonary vascular D. 5. Physical development 6. Conduction disturbance 7. Cardiac function 8. Residual shunting 9. Pulmonary hyperinflation 10. Iatrogenic aortic or tricuspid incompetence 11. Pulmonary hypertension Results of Operation for VSD
Special Situation & Controversies • 1. VSD and patent ductus arteriosus • 2. VSD and coarctation of aorta • 3. Pulmonary artery banding • 4. Approach for conoventricular VSD • 5. Percutaneous closure of VSD • 6. Closure of VSD when PVR is high