Ventricular Septal Defects Transcatheter Closure
1.15k likes | 1.75k Vues
Ventricular Septal Defects Transcatheter Closure. J.V. DeGiovanni Birmingham Children’s Hospital & University Hospital Birmingham UK Advanced Angioplasty 2007. MY CONFLICTS OF INTEREST ARE: Consultant for AGA Medical Corporation Proctor and lecturer for AGA Medical, NMT Medical, WL Gore

Ventricular Septal Defects Transcatheter Closure
E N D
Presentation Transcript
Ventricular Septal DefectsTranscatheter Closure J.V. DeGiovanni Birmingham Children’s Hospital & University Hospital Birmingham UK Advanced Angioplasty 2007
MY CONFLICTS OF INTEREST ARE: Consultant for AGA Medical Corporation Proctor and lecturer for AGA Medical, NMT Medical, WL Gore Steering Committee member for Helex (Gore), SolySafe (Carag), BioStar (NMT)
Study Details • September 2001 – January 2007 • Total number VSD devices : 160 • Muscular Devices: 59 • Perimembranous Devices: 43 • Post-infarct: 43 • Post-trauma: 3 • Residual post-surgery 12
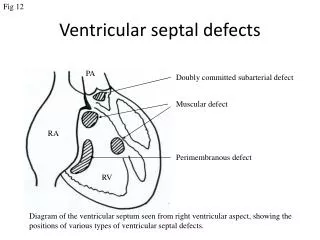
VSD Types • Congenital: Perimembranous, Muscular, Gerbode, Doubly-committed • Acquired: Iatrogenic Residual post-surgery Post-trauma Post-infarct
Indications • Left ventricular volume overload • Heart failure/Cardiogenic shock • Aortic regurgitation • Haemolysis • History of endocarditis • Career reasons • Achieving normality (?)
Technique • General Anaesthesia • Trans-oesophageal echocardiography • Femoral vein/femoral artery • Internal jugular vein/femoral artery • Angiography • +/- Balloon sizing (post-MI only) • Amplatzer device placement and release • Heparin, antibiotics, antiplatelets • Associated procedures (ASD, BAV, RFA, VSD coil, Pulm Valvuloplasty)
Amplatzer Muscular Devices • Muscular Waist diameter 4 – 18 mm Waist length 7 mm Sheath size 6 – 8 Fr • Muscular PI Waist diameter 16 -24 Waist length 10 mm Sheath size 9 – 10 Fr Left disc rim 4 mm, right disc 3mm, size increments 2 mm
Muscular VSDs • Inlet • Muscular/Apical • Outlet
Post-trauman = 3 • Horse Kick, surgery, 3 devices, alive • Bike accident, device closure, alive • Car accident, device pulled through, surgery, died
Post-infarct VSDPatient Details -- ALL • Pt No = 38; Procedures = 43 • Male/Female = 22/16 • Age Range(Mean) = 52 – 81 (68.6 yrs) • Acute/Chronic (First device) = 29/9 • Acute/Chronic (Second device) = 3/2 • Mean Interval between MI and Closure 129 days • Ditto for second device 201 days • Earliest device 2 days, longest 5.3 yrs • Mean Follow-up 18.8 months
VSD Site • Apical 18 • Anterior 6 • Muscular 5 • Inlet/Inferior 9 • Septal aneurysm 6 • Multiple 5 No of defects (No of Pts) 2(2), 3(1), 4(1)
Approach • FA/Jugular 30 • FA/FV 12 • Brachial A/Jugular 1 • Procedure Time 55 – 300 (153) Mins • Fluoro Time 13.6 – 133 (39) Mins • Device size 8 – 24 (18.7)
Planning & Preparation • Maximize fluids and inotropes • IABP but shoot coronaries and consider vital stenting • Allow recovery from reperfusion injury • Early intervention is usually best • Minimize procedural time and trauma • Surgical back-up • Post-Op care • Possible hybrid in some cases