Enclosure 3
Enclosure 3. INTEGRATED PERFORMANCE REPORT for period ending 31 st October 2010 Trust Board – 3 December 2010 - Quality. Appendix 1. Integrated Performance Report: Quality (CO1). Appendix 1. Integrated Performance Report: Quality (CO1). Appendix 1.

Enclosure 3
E N D
Presentation Transcript
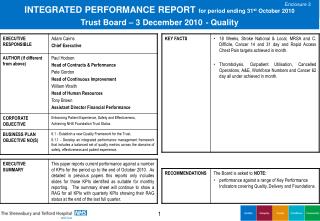
Enclosure 3 INTEGRATED PERFORMANCE REPORTfor period ending 31st October 2010Trust Board – 3 December 2010- Quality
Appendix 1 Integrated Performance Report: Quality (CO1)
Appendix 1 Integrated Performance Report: Quality (CO1)
Appendix 1 Integrated Performance Report: Delivery (CO2, CO3 & CO4)
Appendix 1 Integrated Performance Report: Foundations (CO5 & CO6)
Patient Satisfaction • Actions: • To develop an overarching strategy for collection of patient experience information including patient stories. • A Dignity in Care Conference is being organised in SECC for May 12th 2011 to celebrate Nurses Day .
28 Day Cancelled Operations • Actions: • During October the main causes of patient cancellations were 1) no bed (23 patients) and 2) theatre list overruns (10 patients). The list overruns in the main are due to beds being identified too late during the theatre list. In October there have been a significant number of outliers within the surgical specialities bedbase. • There is a further process mapping session for the Surgical Admission Suite in December, to address some of the patient flow challenges.
Cleanliness • Actions: • Manual system of recording of monitoring used at present. Electronic System to be implemented by January 2011.
Choose and Book • Actions: • Review and action ASIs within the SDUs. 9
End of Life • Actions: • Q3 monitor against baseline. Monthly meeting with clinical coding and palliative care CNS to support data validation. • To take forward recommendations for the development and improvements to Bereavement Services.
Incidents • Actions: • Incident Review Group meets monthly to discuss incidents & trends. Further Root Cause Analysis training for Managers is being planned to improve the consistency of • investigation.
Healthcare Associated Infections (HCAIs) • Actions: • C difficile cluster: An intensive deep clean and review of practice has being carried out. Antibiotic audits are continuing.
Medicines Management • Actions: • Second Audit now completed, results expected to be available at the end of November. • Report to be forwarded to PCT when audit results are available. • Action plan to be further developed dependent on audit results.
Patient Falls • Actions: • Falls information on Internet and Intranet. • To undertake further in depth analysis on falls data and categories. • Ward Managers and Matrons to be alerted to falls on daily basis so more proactive and immediate review can take place.
Hospital Standardised Mortality Ratio (HSMR) • Actions: • Senior nurses will be trained in the use of the Global Trigger Tool in December. • A coding workshop was held on 15th October. A number of Clinicians have been identified as ‘Coding Champions’. A further workshop will be held in November. • The Trust is working with the University of Birmingham to understand the data more fully; develop an alternative system for monitoring deaths, and to set up a research • project.
Stroke • Actions: • Data Analyst interviews to take place on Friday November 5th. • Thrombolysis Service to commence seven days a week 08:00 – 20:00 at both PRH and RSH from December 6th (Phase One). • Hyper acute Stroke patients (including Thrombolysis) to be provided at one site only (PRH) during hours 20:00 – 08:00 from January 5th (Phase Two – Interim phase). • Option appraisal to be carried out during March 2011 (re. Phase Two). • Implement a twenty-four/seven service to include Thrombolysis at a single site (Phase Three).
Stroke - CQUIN Actions:
Early Access to Maternity • Actions: • Review of database to identify specific GP practices referring pregnant women late to Maternity Services. • Review of database to identify midwives undertaking booking assessment outside of target (following appropriate referral into the system). • Recruitment to midwifery vacancies within PRH to be tightly managed.
Nutrition • Actions: • Further expansion of Protected Meal Times implementation to commence from September 2010. • Nutritional Steering Group members to visit Trust in the Region who have successfully implemented Protected Meal Times.
Readmission Rates Actions:
Venous Thromboembolism • Actions:
Think Glucose • Actions: • Continuation of delivery of action plan. • Plan to roll out pre filled insulin syringes during January. • Develop audit tool to measure compliance.
Tissue Viability • Actions: • RCA training arranged in November for Ward Managers . • Continue with education roll out. • To review Trust wide Prevalence audit results.
Appraisals • Actions: • Departments falling below 60% are performance managed by the relevant Executive Director.
Smoking Actions:
Staying Healthy (Alcohol) - CQUIN • Actions: • 9a: There are significant concerns around the delivery of IBA after April 2011 at RSH due to resourcing Alcohol specialist post. CQUIN uplift payments are required to assist in service • provision and agreement of this needs to allow for 3 months to ensure continuity and training. • 9b: Delay in agreement for SLA across providers/commissioners. The need for this is agreed and will be written by PCT’s in discussion with acute Trust. This is not totally in the control of the CQUIN group.
Care Quality Commission Registration • Actions: • Lead Managers have been asked to submit evidence of continuing compliance against the Essential Standards of Quality and Safety for Quarter 2. • Internal Audit will be auditing the evidence of compliance in November.
Coding • Actions: • The Clinical Coding Manager continues to audit the recording of co-morbidities on a monthly basis making use of the Coding analytics software.
A&E 4 Hour Waits • Actions: • Daily Conference Calls continue. • Health and Social Care Winter Planning commenced. • Urgent Care Network Review and relaunch.
18 Weeks Actions:
14 Day Cancer • Actions: • The 14 day target has improved significantly and has been sustained over the past few weeks. This is due to the additional capacity which is now available within the Breast Service to • ensure patients are offered the choice of two dates. We are continuing to work closely with the PCTs and auditing the patients that choose not to accept an appointment within 14 days and • looking into each case individually. In order to establish why patients are choosing to wait longer than 14 days, we are telephoning patients to establish the reason why. • Demand and capacity for all specialities has been audited over the last 12 months and processes are being put in place to increase capacity where appropriate because from 1st December 2010 all two week wait appointments will be on Choose and Book.
31 Day Cancer • Actions: • Although not consistently, we have previously met this target and have gone over and above it. Our aim is to meet this target consistently by the end of December 2010. We have both capacity & staffing issues within Radiotherapy Department which have been acknowledged. The number of Oncologists employed has increased and therefore the demand for access to the radiotherapy machines has increased and plans have been agreed to increase radiography and physics staffing to increase linac capacity in line with NRAG recommendations.
62 Day Cancer • Actions: • In order to improve and maintain the delivery of the 62 day target, the pathway for Upper GI patients will be re-designed to improve the current delays. This work is being coordinated by the Service Improvement Nurse within Cancer Services. Changes made within the Administration Team will ensure that all patients are tracked correctly to ensure there are no delays. • Work is starting in December with the Department of Health Intensive Support Team to identify areas for improvement.
Thrombolysis • Actions: • Internal systems and processes for the delivery of thrombolysis in A&E and the management of acute chest pain admissions ongoing. • Chest Pain direct admission to CCU project initiated, awaiting outcome report.
Rapid Access Chest Pain Actions: