Download
1 / 34
350 likes | 915 Vues
Hereditary Hemochromatosis. Prepared by: Sean Blaine BSc, MD, CCFP Family Physician - Stratford, Ontario Assistant Professor, University of Toronto June C Carroll MD, CCFP, FCFP Sydney G. Frankfort Chair in Family Medicine Mount Sinai Hospital , University of Toronto

E N D
Hereditary Hemochromatosis Prepared by: Sean Blaine BSc, MD, CCFP Family Physician - Stratford, Ontario Assistant Professor, University of Toronto June C Carroll MD, CCFP, FCFP Sydney G. Frankfort Chair in Family Medicine Mount Sinai Hospital, University of Toronto Andrea L Rideout, MS, CGC, CCGC Certified Genetic Counsellor Project Manager – The Genetics Education Project Funded by: Ontario Women’s Health Council Version: February 2006
Acknowledgments • Reviewers: Members of The Genetics Education Project • Funded by: Ontario Women’s Health Council as part of its funding to The Genetics Education Project * Health care providers must use their own clinical judgment in addition to the information presented herein. The authors assume no responsibility or liability resulting from the use of information in this presentation.
Outline • Hereditary hemochromatosis • Clinical picture • Symptom/pattern recognition • When to offer testing • Benefits, risks & limitations of genetic testing • Management recommendations
What Is Hemochromatosis ? • Disorder of iron overload • Hereditary hemochromatosis (HH) • Acquired hemochromatosis • HH: genetic defect in iron metabolism • Excess iron absorbed from the gut • Symptoms due to pathologic deposition of iron in body tissue = iron overload
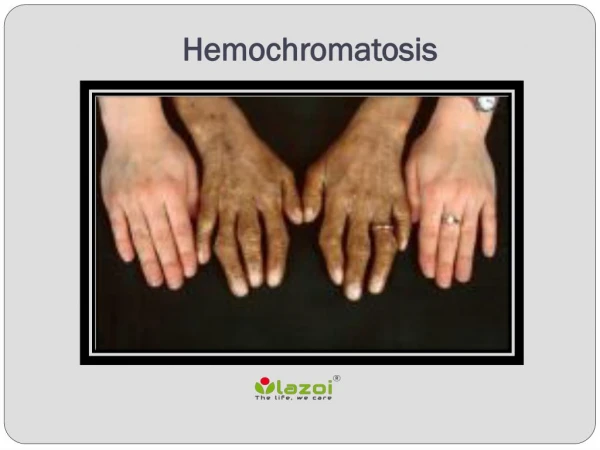
Symptoms – Traditional Concept • Classic Triad: • Cirrhosis (hepatic damage) • Diabetes (type II) (pancreatic damage) • Bronzing of skin (hyperpigmentation) • Traditional triad means diagnosed too late! • Damage may be only partially reversible • Goal is to detect the disease BEFORE organ damage occurs
Non-Specific Symptoms and Signs • Liver: hepatomegaly, elevated liver enzymes • Cardiac: myocardial infarction, cardiomyopathy • Endocrine: impotence/amenorrhea, diabetes • Musculoskeletal: arthritis/arthralgia • Fatigue: unexplained, severe and chronic Generally not evident until 40-60 years of age Some patients may present earlier
The Genetics of Hemochromatosis • HFE– associated Hemochromatosis accounts for > 90% of cases and is the most common adult onset form: • Autosomal recessive inheritance • C282Y mutation • Carrier rate 1 in 7 - 10 Caucasians • Incidence 1 in 200 - 400 • Penetrance is low
Autosomal Recessive Inheritance • Legend • B:Normal HFE gene • b: HFE gene with mutation Unaffected Carrier Unaffected carrier Bb Bb BB Bb Bb bb Unaffected Susceptible genotype for Hemochromatosis Unaffected carrier Unaffected carrier
The HFE Gene • HFE gene on chromosome 6 • Involved in iron homeostasis • HFE protein normally limits amount of iron uptake by gut and regulates amount of iron stored in the tissues • Two common mutations in HFE • C283Y allele • H63D allele • HFE gene mutations produce altered HFE protein unable to properly regulate iron metabolism - results in an excess of iron storage in tissues
Case • Seamus, 60 y.o. male: • 3 month history of fatigue & joint pain • drinks 2 beers/day • brother with type 2 diabetes • Physical exam: • hepatomegaly • enlarged and tender knuckles • several tattoos
Seamus’ routine blood work: Fasting glucose - normal Bilirubin - normal ALT 67 U/L (reference range 0-40) AST 73 U/L (reference range 0-37) GGT 92 U/L (reference range 5-35) Seamus stops drinking, 6 weeks later: ALT & AST levels are unchanged GGT - normal Hepatitis A & B serology negative What next? Case
Case • Further blood work: • Ferritin 640 mcg/L(reference range <300mcg/L) • Transferrin saturation 60% (reference range <45%) • What is the diagnosis?
Consider Hemochromatosis! In symptomatic patients with: • Unexplained liver disease, with abnormal serum iron markers • Type II diabetes particularly with: • Hepatomegaly, elevated liver enzymes, atypical cardiac disease, early onset sexual dysfunction • Early onset arthropathy, cardiac disease, male sexual dysfunction
Consider Hemochromatosis! In asymptomatic patients with: • Unexplained elevation of liver enzymes or asymptomatic hepatomegaly • Abnormal serum iron markers on routine blood work • Lethargy/fatigue • First degree relatives of a confirmed HH case
Diagnostic testing for HH • Transferrin saturation: • >45% indicates significant Fe accumulation • Serum ferritin -levels indicating significant iron accumulation: • >200 mcg/L pre-menopausal women • >300 mcg/L post-menopausal women • >300 mcg/L for men • Liver biopsy if ferritin >1000 to assess damage Consider genetic testing – DNA testing for common mutations (C282Y, H63D)
Genetic Testing for HHShould be offered to those patients with: • Appropriate clinical presentation • Elevated transferrin saturation and ferritin • Liver biopsy suggestive of iron overload • First degree relative of a known case *Must be offered to an affected family member or index case FIRST • A known mutation should be identified before offering DNA testing to other family members
What is the value of genetic testing? • To confirm diagnosis • Sequential screening of family members • Family members with identified mutations can be offered: • Screening plan to monitor for iron overload. • Normal life expectancy if diagnosed before DM or cirrhosis • Treatment plan to prevent further organ damage, morbidity & mortality. • Prolonged survival with serial phlebotomy • Goal of ferritin <50 may take > 1 year • Environmental modification • Diet, alcohol, viral hepatitis A/B immunization
Discussing Genetic Testing • Informed choice • Risks, benefits & limitations of testing • Walk patient through various scenarios • Positive test result • Negative test results • Psychosocial issues: self-concept, insurance discrimination, family issues, non-paternity OR Refer to your local Genetics Clinic
Case (cont.) • Seamus decides to have genetic testing • Genetic testing for Seamus shows • HFE: C282Y/C282Y (homozygote) • This is the susceptible genotype and Seamus has hemochromatosis • After 6 months of weekly phlebotomy his liver function parameters normalize • Let’s look at his family history…
Legend CA liver Arthritis IDDM 3 3 N 3 Seamus’ Family History Ireland/Ireland Germany/England CA- Liver - 69 ‘old age’ - 80 WW II Alzheimer disease - 95 Seamus -60 Arthritis - 64 All A&W Heidi -55 A&W Accident -21 A&W -65 Diabetes -69 A&W - 62 Diabetes - 55 All A&W All A&W All A&W A&W Angela – 13 A&W Both A&W
Genetic testing of minor children • Seamus and his wife request HH testing for their 13 year old daughter. • Would you offer their daughter testing? • Consider potential benefits and harms: • Medical issues • Psychosocial issues • Reproductive issues • For adult onset conditions it is generally accepted that the child make a decision after they reach the age of understanding and the capacity to give consent - generally adulthood.
More consequences of having a mutation • Research shows very few negative emotional consequences to having a HH mutation • Potential consequences: • anxiety, depression or relief • positive health behaviour may be reinforced • may develop fatalistic attitude toward to health • insurance discrimination • Unanticipated outcomes • i.e. nonpaternity
“So if I have the gene…I’ll get the disease” • Not necessarily! • This statement refers to an important concept in genetics • Penetrance • The proportion of individuals with a mutation causing a particular disorder who exhibit clinical symptoms of that disorder
Mutated HFE Genes = Hemochromatosis? No, because of • Incomplete penetrance: • Even though some individuals have the susceptible genotype they may never manifest symptoms of the disease due to: • Environmental factors: blood donation • Genetic factors: other modifying genes • Low penetrance for C282Y homozygotes
Medical Management • The goal - detect patients before symptoms of iron overload. • Phlebotomy weekly or biweekly • Check ferritin every ~10 phlebotomies • Stop frequent phlebotomy when ferritin 25-50mcg/L • Maintenance phlebotomy every 3-4 months • Dietary recommendations • Consider hematology or GI consult for confirmed cases to guide treatment and monitoring
Summary • Think genetically! • Three generation family history • Risks, benefits & limitations of genetic testing • HH Pattern recognition • Multiple signs, symptoms, and disease manifestations may be a clue to early diagnosis • HH Goal: detect and treat affected individuals before signs of organ damage
Resources • The Canadian Hemochromatosis Society: • http://www.cdnhemochromatosis.ca/main.htm • Gene Reviews: http://www.genetests.org/ • See HFE-associated Hemochromatosis • Iron Disorders Institute website: • http://www.irondisorders.org/ • Review article from the American College of Gastroenterology: • Adams P et al. EASL international consensus conference on haemochromatosis. J Hepat. 2000; 33:485-504. • Tavill AS et. al Diagnosis and management of hemochromatosis. Hepatology. 2001;33:1321-1328. • Contact your local genetics centre • http://www.cagc-accg.ca/centre1.html
June Carroll MD CCFP Judith Allanson MD FRCP FRCP(C) FCCMG FABMG Sean Blaine MD CCFP Mary Jane Esplen PhD RN Sandra Farrell MD FRCPC FCCMG Judy Fiddes Gail Graham MD FRCPC FCCMG Jennifer MacKenzie MD FRCPC FAAP FCCMG Wendy Meschino MD FRCPC FCCMG Joanne Miyazaki Andrea Rideout MS CGC CCGC Cheryl Shuman MS CGC Anne Summers MD FCCMG FRCPC Sherry Taylor PhD FCCMG Brenda Wilson BSc MB ChB MSc MRCP(UK) FFPH The Genetics Education Project Committee
References • Dooley J. Diagnosis and management of genetic haemochromatosis. Best PractRes Clin Haematol. 2002; 15:277-293. • Borgaonkar MR Hemochromatosis more common than you think. Can Fam Physician 2003; 49:36-43. • Pietrangelo A. Hereditary Hemochromatosis- a new look at an old disease NEJM 2004; 350:2383-2397. • Cazzola M. Genetic disorders of iron overload and the novel “ferroportin disease.” Haematologica 2003; 88: 721-724.
References • Adams P et al. EASL international consensus conference on haematchromatosis. J Hepat. 2000; 33:485-504. • Olynyk JK, Cullen DJ Aquilia A et al. A population study of the clinical expression of the hemochromatosis gene. NEJM 1999; 341:718-724. • Worwood M. Genetics of Haemochromatosis. Bailleres Clin Haemtol. 1994; 7:903-18. • Milman N, Pedersen P, Steig T, Melsen GV. Frequencies of the hereditary hemochromatosis allele in different populations. Comparison of previous phenotypic methods and novel genotypic methods.Int J Hematol. 2003; 77: 48-54.
References • Feder JN, Gnirke A Thomas W et al. A novel MHC class I-like gene is mutated in patients with hereditary hemochromatosis. Nat Genet. 1996; 13:399-408. • Borwein S Ghent CN Valberg LS. Diagnostic efficacy of screening for hereditary hemochromatosis. Can Med Assoc J 1984; 131:89901. Adams PC Chakrabarti S. Genotypic/phenotypic correlations in genetic hemochromatosis: evolution of diagnostic criteria. Gastroenterology. 1998; 114:319-323. • Ramrakhiani S, Bacon BR. Hemochromatosis: Advances in Molecular genetics and clinical diagnosis. J Clin Gastroenterol 1998; 27:41-46.
References • Jackson HA, Carter K, Darke C et al. HFE mutations, iron deficiency and overload in 10 500 blood donors. Br J Haematol 2001; 114:474-484. • Tavill AS Diagnosis and management of hemochromatosis. Hepatology 2001; 33: 1323-1328. • Canadian College of Medical Genetics. Position statement – genetic testing of children November 26, 2000. • American College of Medical Genetics. Genetic testing in children and adolescents, points to consider: ethical, legal and psychological implications of (ACMG/ASHG). Am J Hum Genet 57:1233-1241.
References • Beutler E, Felitti VJ, Koziol JA, Ho NJ, Gelbart T. Penetrance of 845G→A (C282Y) HFE hereditary haemochromatosis mutation in the USA. Lancet 359:211-218. • Patch C, Roderick P, Rosenberg W. Comparison of genotypic and phenotypic strategies for population screening in hemochromatosis: Assessment of anxiety, depression, and perception of health. Genet Med 2005; 7:550-556. • Gordon RS, McManus. From the NIH Highly invasive new bacterium isolated from US east coast waters. JAMA. 1984; 251: 323-325.