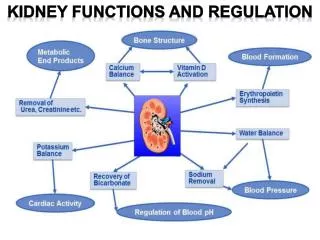
Kidney Functions
Kidney Functions. Filter 200 liters of blood daily, allowing toxins, metabolic wastes, and excess ions to leave the body in urine Regulate volume and chemical makeup of the blood Maintain the proper balance between water and salts

Kidney Functions
E N D
Presentation Transcript
Kidney Functions • Filter 200 liters of blood daily, allowing toxins, metabolic wastes, and excess ions to leave the body in urine • Regulate volume and chemical makeup of the blood • Maintain the proper balance between water and salts • Production of rennin to help regulate blood pressure and erythropoietin to stimulate RBC production • Adjust blood pH when other buffer system are insufficient
Kidney Function Table 19-1
The Filtration Fraction 4 >99% of plasmaentering kidneyreturns to systemiccirculation. Efferent arteriole Peritubularcapillaries 5 <1% ofvolume isexcreted toexternalenvironment. 80% 2 20% ofvolumefilters. >19% of fluidis reabsorbed. 3 Afferentarteriole Bowman’scapsule Remainderof nephron 1 Plasma volumeentering afferentarteriole = 100% Glomerulus Figure 19-4
Nephrons • Each kidney contains over million nephrons – the anatomical units responsible for urine formation. Nephron functions include • Production of filtrate • Reabsorption of organic nutrients, water and ions • Secretion of waste products into tubular fluid
Nephron’s parts • Consists of 2 parts: • The renal corpuscle which is the location of blood filtration – in the cortex • The renal tubule is the location of filtrate processing into urine – in cortex and medulla
The nephron Bowman’scapsule Proximal tubule Distal tubule Ascendinglimb of loopends Descendinglimb of loopbegins Renal corpuscle Collectingduct Renal tubules Collecting system Descendinglimb Ascendinglimb (j) Parts of a nephron Loop ofHenle To Minor calyx To bladder Figure 19-1j
Nephrons’ location • Cortical nephrons – 85% of nephrons; located in the cortex • Juxtamedullary nephrons: • Are located at the cortex-medulla junction • Have loops of Henle that deeply invade the medulla • Have extensive thin segments • Are involved in the production of concentrated urine
Glomerulus – site of blood filtration • Several small arterioles exit from the cortical radiate arteriole – afferent arterioles • Each afferent arteriole folds to create a “little ball”– the glomerulus • The blood from the glumerulus is carried out by efferent arteriole • The capillaries in the glomerulus are found between 2 arteries • the efferent arteriole enters into a regular capillary bed – peritubular capillaries
Mechanisms of Urine Formation • The kidneys filter the body’s entire plasma volume 60 times each day • The filtrate: • Contains all plasma components except protein • Loses water, nutrients, and essential ions to become urine • The urine contains metabolic wastes and unneeded substances
Basic processes of urine formation • Glumerular Filtration • The fluid that is forced out of capillaries into the Bowman’s space is called glumerular filtrate • Similar to blood plasma without the proteins • Tubular reabsorption and secretion • The fluid in the tubules is called tubular fluid • Differs from the filtrate because substances are moving in and out the tubules • Water conservation • Occur in the collecting duct • The fluid is called urine
Kidney Function • The urinary excretion of substance depends on its filtration, reabsorption, and secretion Glomerulus Efferentarteriole Peritubularcapillaries To renal vein Tubule Afferentarteriole Bowman’scapsule To bladder andexternal environment Amountreabsorbed Amountfiltered Amountsecreted amount of soluteexcreted – = + Figure 19-3
Nephron’s parts – structure and function • Consists of 2 parts: • The renal corpuscle which is the location of blood filtration – in the cortex • The renal tubule is the location of filtrate processing into urine – in cortex and medulla
The Renal Corpuscle Podocyte Lumen ofBowman’scapsule Glomerularcapillary Podocytefootprocesses Capillaryendothelium Mesangialcell (c) Podocyte foot processes surround eachcapillary, leaving slits through which filtrationtakes place. Figure 19-5c
Glomerular filtration membrane • Fluid from capillaries need to pass through 3 barriers to get to the capsular space: • Fenestrated endothelium of capillaries with pores that allow the passage of relatively large molecules but not blood cells (pores size – 60-100nm) • In addition, endothelial cells have negatively charged glycoproteins on their surface that “deny” entrance of negatively charged molecules • Basement membrane – negatively charged proteins that do not allow the passage of large and negatively charged molecules (stop molecules >8nm)
Glomerular filtration membrane • Filtration slits – form by the pedicles of the podocyes that create filtration slits (slit size 6-9nm). Filtrate on basis of size and negative charge • Water and some solutes pass from blood plasma in the glomerulus capillaries to the capsular space of the nephrone • Molecules smaller than 3 nm in diameter (water, sodium, glucose, amino acids, nitrogen wastes) pass freely from blood into capsule
The Renal Corpuscle Foot processof podocyte Filtration slit Pores inendothelium Basal lamina Capillarylumen Filteredmaterial Lumen ofBowman’scapsule (d) Filtered substances passthrough endothelial poresand filtration slits. Figure 19-5d
Most molecules smaller than 3 nm can pass freely. That includes water, electrolytes, glucose, fatty acids, amino acids, nitrogenous wastes and vitamins http://members.aol.com/Bio50/LecNotes/lecnot37.html
Nephron’s parts - the tubules – reabsorption and secretion • The renal tubule is the location of filtrate processing into urine • It is consists of • Proximal convoluted tubule (PCT) • Loop of Henle • Distal convoluted tubule (DCT)
Glomerular Filtration • Filtration is a passive process in which hydrostatic pressure forces fluid and solutes through a membrane • The glomerulus is more efficientthan other capillary beds because: • Large surface area of the filtration membrane • filtration membrane is more permeable • Glomerular blood pressure is higher because • Arterioles are high-resistance vessels • Afferent arterioles have larger diameters than efferent arterioles • Higher BP results in higher net filtration pressure
Glomerular filtration depends on pressures • Filtration depends on the balance between hydrostatic pressure and colloid osmotic pressure on both sides of the capillary wall • Blood hydrostatic pressure (BHP) is much higher in the glomerulus (60 mmHg as compared to 10-15) • Hydrostatic pressure in the capsular space is about 18 mm Hg (compared to about 0 in the interstitial fluid). • This is a result of continuous filtration and the presence of fluid in the space. • The colloid osmotic pressure (COP) of the blood is about the same as elsewhere – 32 mm Hg • The glomerular filtrate is almost protein-free and has no significant COP
Glomerular filtration • Total forces in the renal corpuscle: • Forces that work to move fluid from capillaries into capsular space: • Glomerular capillaries hydrostatic pressure (GHP) – 55-60 mm Hg • Forces that work to move fluid out of capsular space to capillaries: • Blood colloid osmotic pressure (BCOP) – 32 mm Hg • Capsular space hydrostatic pressure (CsHP) – 18 mm Hg • 60 out – 18 in – 32 in = 10 mmHg net filtration pressure
Glomerular filtration rate (GFR) • Amount of filtrate produced by the two kidneys each minute (~125 ml) • Factors that control GFR: • Total surface area available for filtration • Filtration membrane permeability • Net filtration pressure (NFP) • GFR is usually measured over 24 hr and it is about 180 L/day for males and 150 L/day in females
Regulation of Glomerular Filtration rate • 2 types of mechanisms control the GFR • Renal autoregulation (intrinsic system) • Tubuloglomerularfeedback mechanism • Myogenic mechanism • Extrinsic mechanisms • Neural controls (extrinsic system) • Hormonal mechanism (the renin-angiotensin system)
Intrinsic Controls - autoregulation • Renal autoregulation is the ability of the nephron to adjust the blood flow and GFR without external control • Under normal conditions, renal autoregulation maintains a nearly constant glomerular filtration rate • Autoregulation involves two types of control • Flow-dependent tubuloglomerular feedback – senses changes in the juxtaglomerular apparatus • Myogenic – responds to changes in pressure in the renal blood vessels
Tubuluglomerular feedback mechanism • The juxtaglomerular apparatus (JGA) monitors the fluid entering the DCT and adjusts the GFR • Components of the JGA: • The granular/juxtaglumerular (JG) cells – enlarged smooth muscle cells in the afferent arteriole. • They respond to the cells of the macula densa to dilate or constrict the arterioles • Act as mechanoreceptors that sense blood pressure • Can release renin when BP decrease • The macula densa is a patch of ET at the start of the DCT (in some books it said to be in loop of Henle) directly across from the JG cell • Sense NaCl concentration in the tubular fluid
Autoregulation control of GFR • If GFR rises, flow of tubular fluid increases and rate of NaCl reabsorption decreases. • The macula densa sense the change and stimulate the contraction of JG cells • This results in constriction of the afferent arteriole thus reducing GFR
Intrinsic Controls: Myogenic Mechanism • The myogenic mechanism – base on the tendency of smooth muscle to contract when stretches • BP constriction of afferent arterioles • Helps maintain normal GFR • Protects glomeruli from damaging high BP • BP dilation of afferent arterioles • Helps maintain normal GFR
Tubuloglomerular Feedback Glomerulus Distal tubule 1 GFR increases. Efferent arteriole 2 Flow through tubule increases. Bowman’s capsule 3 4 Flow past macula densa increases. 1 Macula densa 5 Granular cells 4 Paracrine from maculadensa to afferent arteriole Afferent arteriole 2 3 Proximaltubule 5 Afferent arteriole constricts. Resistance in afferentarteriole increases. Collectingduct Hydrostatic pressurein glomerulus decreases. LoopofHenle GFR decreases. Figure 19-10, steps 1–5 (4 of 4)
Filtration • Autoregulation of glomerular filtration rate takes place over a wide range of blood pressures Figure 19-7
Extrinsic Controls – neural control • When the sympathetic nervous system is at rest: • Renal blood vessels are maximally dilated • Autoregulation mechanisms is controlling • Under stress: • Norepinephrine is released by the sympathetic nervous system • Epinephrine is released by the adrenal medulla • Afferent arterioles constrict and filtration is inhibited • The sympathetic nervous system also stimulates the renin-angiotensin mechanism
Renin-Angiotensin Mechanism – hormonal control • A reductionin afferent arteriole pressure triggers the JG cells release renin • Renin acts on angiotensinogen to release angiotensin I • Angiotensin I is converted to angiotensin II • Angiotensin II: • Causes mean arterial pressure to rise • Stimulates the adrenal cortex to release aldosterone • As a result, both systemic and glomerular hydrostatic pressure rise
Extrinsic Controls: Renin-Angiotensin Mechanism • Triggered when the granular cells of the JGA release renin angiotensinogen (a plasma globulin) resin angiotensin I angiotensin converting enzyme (ACE) angiotensin II
Renal tubules function - Reabsorption and secretion • Conversion of the glomerular filtrate to urine involves the removal and addition of chemicals by tubular reabsorption and secretion • Reabsorption – from tubules back to the blood stream • Secretion – from blood stream to tubules (not part of filtration) • Cells of the PCT reabsorb 60-70% of the filtrate volume
Non-reabsorbed Substances • Substances are not reabsorbed if they: • Lack carriers • Are not lipid soluble • Are too large to pass through membrane pores
Nonreabsorbed Substances • A transport maximum (Tm): • Reflects the number of carriers in the renal tubules available • Exists for nearly every substance that is actively reabsorbed • When the carriers are saturated, excess of that substance is excreted
Transport maximum (Tm) and the Renal Threshold • If nutrient concentrations rise in tubular fluid: • Reabsorption rates increase until carrier proteins are saturated • Concentration higher than transport maximum: • Exceeds reabsorptive abilities of nephron • Some material will remain in the tubular fluid and appear in the urine • Determines the renal threshold
Glucose Reabsorption • Carrier proteins for glucose reabsorption • Apical membrane: secondary active transport • Basolateral membrane: facilitated diffusion
The loop of Henle - Regulation of Urine Concentration and Volume • Osmolality • The number of solute particles dissolved in 1L of water • Reflects the solution’s ability to cause osmosis • Body fluids are measured in milliosmols (mOsm) • The kidneys keep the solute load of body fluids constant at about 300 mOsm • This is accomplished by the countercurrent mechanism
The loop of Henle and countercurrent multiplication • Countercurrent multiplication– exchange occurs between fluids moving in different directions; the effect of the exchange increased as the fluid movement continues • Between the close ascending and descending limbs of loop • Difference in permeability in two arms: • Thin descending is permeable to water and almost not to solutes • Thick ascendingrelatively impermeable to both but contains active transport mechanism that pump sodium and chloride ions from tubular fluid to peritubular fluid of the medulla
Countercurrent multiplication • Sodium and chloride are pumped out of the thick ascending limb into the peritubular fluid by co-transport carriers (Na+-K+/2Cl- transporter) • That elevates the osmotic concentration in the peritubular fluid around the thin descending limb • The result is flow of water out of the thin descending limb into the peritubular fluid and increased concentration of solutes in the thin limb • The arrival of highly concentrated solution in the thick limb accelerate the reabsorption of sodium and chloride ions
Countercurrent Multiplication and Concentration of Urine Figure 26.13b
Osmolality of interstitial fluid (mOsm) Filtrate entering the loop of Henle is isosmotic to both blood plasma and cortical interstitial fluid. H2O NaCI Cortex Active transport Passive transport NaCI H2O Water impermeable NaCI H2O NaCI H2O The descending limb: • Permeable to H2O • Impermeable to NaCl As filtrate flows, it becomes increasingly concentrated as H2O leaves the tubule by osmosis. The filtrate osmolality increases from 300 to 1200 mOsm. Outer medulla H2O NaCI H2O H2O Inner medulla Loop of Henle The ascending limb: • Impermeable to H2O • Permeable to NaCl Filtrate becomes increasingly dilute as NaCl leaves, eventually becoming hypo-osmotic to blood at 100 mOsm in the cortex. NaCl leaving the ascending limb increases the osmolality of the medullary interstitial fluid. (a) Countercurrent multiplier. The long loops of Henle of the juxtamedullary nephrons create the medullary osmotic gradient. Figure 25.16a
The countercurrent multiplication: • Creates osmotic gradient in medulla • Facilitates reabsorption of water and solutes before the DCT • Permits passive reabsorption of water from tubular fluid in the collecting system