Functions of the Kidney
420 likes | 630 Vues
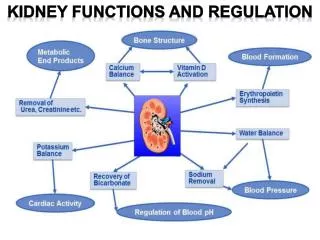
Functions of the Kidney. Maintain electrolyte, acid-base balance “clear” the blood of toxins Make EPO, active Vitamin D gluconeogenesis, hormone metabolism. Hyponatremia Hypokalemia Metabolic Alkalosis chloride responsive chloride unresponsive Metabolic Acidosis anion gap non-anion gap.

Functions of the Kidney
E N D
Presentation Transcript
Functions of the Kidney • Maintain electrolyte, acid-base balance • “clear” the blood of toxins • Make EPO, active Vitamin D • gluconeogenesis, hormone metabolism
Hyponatremia Hypokalemia Metabolic Alkalosis chloride responsive chloride unresponsive Metabolic Acidosis anion gap non-anion gap Hypernatremia Hyperkalemia Calcium Phosphate Magnesium Kidney disorders
Renal Failure • A growing epidemic • 350,000 on renal replacement therapy • 80-90,000 new every year • Over one million thought to be in pipeline
Creatinine • Normal 0.8-1.2mg/dl; lower in pregnancy and cirrhosis and chronically ill/aged, higher in muscleheads, pts taking creatine and in rhabdo. • Cephalosporins/ketosis change assay to increase creat, cimetidine and trimethoprim block secretion to increase
BUN • Normal 5-10mg/dl • Increased with GFR, heavy GI bleed, TPN, hypercatabolic states (steroids, sepsis) and prerenal volume depletion-( >20x creat), such as CHF, cirrhosis, nephrosis, sepsis and salt depletion. • When >100mg/dl, often associated with uremia
Hematuria • Definition • straightforward- >3-5 RBC’s per high power field • Definitions may vary
Causes of hematuria • Anatomic • Kidney • Ureters • Bladder • Urethra • Prostate or GYN
Proteinuria • Microalbuminuria-dip (-), 30-300 mg/day of albuminuria. Seen in diabetes, vascular dz • Dip(+) urine, 300mg-2 g seen in glomerular and tubular disease • Dip (+) urine, > 2g/day, glomerular disease • Dip (-) urine, still can be overflow protein from myeloma, use SSA or UPEP
Hypertension • Defined as resting, repeated BP > 140/90 • Risk parallels severity of increased BP and other risks for vasc. Dx-male, AA, smoking, diabetes, cholesterol, age • Treat mild BP with diet, weight loss, exercise • Move onto drugs when above fails • Approx 5% of pts have secondary causes, more when BP severely elevated
HTN- secondary causes • Truncal obesity- Cushing’s • Labile HTN - Pheo • Bruits- Renal artery stenosis • Decreased fem pulses- Coarctation • Abdominal/flank mass- Polycystic kidneys • Increased creat/edema- Renal disease • Hypercalcemia- Hyperparathyrodism • Hypokalemia- Hyperaldosteronism/licorice/ Liddle’s syndrome
HTN- Rx • Diabetics, renal disease with proteinuria, Cardiac injury- ACE inhibitors • Must watch for reversible hyperkalemia, renal insufficiency, cough, angioedema • Think bilateral renal artery stenosis when acute renal failure occurs. • Do not use ACEi or ARBs in pregnancy
Glomerular disease • Hematuria, proteinuria or both • RBC casts, especially when proliferative • Nephritis: hematuria, hypertension, renal insufficiency and edema • Nephrosis; proteinuria (nephrotic>3.5g/d) with edema, hypoalbuminemia and hypercholesterolemia • Idiopathic or part of systemic disease
Chronic renal failure • Diabetes • HTN • Glomerular disease (IgA, membranous, FSGS) • PCKD • SLE • Interstitial disease • Heriditary/ Congenital
PKD • Autosomal dominant (1 in 800) • > 2 cysts/kidney by age 30 • Large cysts with chance of infection/hemorrhage, assoc with berry aneurysm, diverticulosis, floppy valves, other organ cysts (liver/panc/ovarian) • Treat infection with Cipro • NO Rx for disease yet
Interstitial disease • Reflux nephropathy with pyelo • NSAIDS/TYLENOL/Pb/heavy metals • SLE/Sjogren’s/Sarcoid/TB • Chinese herbs • Usually mild HTN, mild proteinuria, pyuria • hypercalcemia for granulomatous disease
Chronic renal failure • Clearance- if inadequate, dialysis/transplant • Anemia- normochromic,normocytic treated with EPO and iron • Bones- high phos and low Vit D cause low Ca++, high PTH--Rx with PO4 binders and Vit D • Access- potential for steal/infection/high output heart failure
Stalling ESRD • Blood pressure control • ACE inhibitors/ ESRD • Low salt, low protein diet • ? Treatment of underlying disease • Preventing toxicities
Treating anemia • Improves energy, sexual function, mentation, quality of life and possibly reduces LVH, angina, death • Effective treatment with iron, EPO, NESP • Careful to screen for other causes of anemia
Protecting the bones • Limit phosphate intake • Phosphate binders • Calcium or Renagel • Vitamin D • Monitor labs
Protect the heart?? • Exercise • Healthy diet • NO SMOKING, Limited EtOH • ? Lipid management • ?Aspirin
Dialysis • Start for low clearance, esp if poor nutrition • Outcome marker is albumin • Hemodialysis most common, initial comp is dysequilibrium from rapid decrease of osmolality. Chronic complications of hypotension and cramping, arrythmia • Death from heart disease, infection, cancer, access failure, discontinuation
Peritoneal dialysis • Must do large volume, frequent exchanges for adequacy • Less anemia and high blood pressure • Peritonitis less common but still well represented. Usually Staph (70-80%) or E. coli (15-20%). Rarely fungal • Treat with appropriate antibiotic IP, pull catheter if fungal or fails RX
Transplant • Highly effective- 90 % 1 year success • LRD>CAD • Problems are immunosuppression, rejection • Infections are early bacterial (post-op), viral after 1 month (CMV), PCP in first year;prophylaxis effective • Technical problems;obstruction and renal artery stenosis have usual sequelae/RX
Transplant • Loss of kidney function • Death (cards late, infection early) • Chronic rejection • Cyclosporine toxicity • Recurrent disease • FSGS, MPGN, membranous, IgA, oxalosis • NOT heriditary disease (PKD, cystinosis, Alport)