Download
1 / 122
1.22k likes | 2.22k Vues
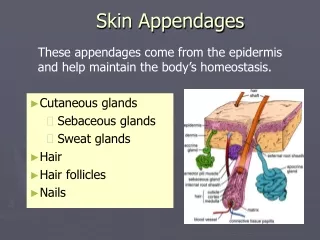
Diseases of the Skin Appendages. Adam Wray, D.O. September 13, 2005. Non-scarring alopecias. Alopecia areata. Characterized by rapid and complete loss of hair in one or more often several round or oval patches

E N D
Diseases of the Skin Appendages Adam Wray, D.O. September 13, 2005
Alopecia areata • Characterized by rapid and complete loss of hair in one or more often several round or oval patches • “Exclamation point” hairs that are tapered at the base may persist in localized patches • Usually on the scalp, bearded areas, eyebrows and eyelashes • 1-5 cm • May progress to total loss of scalp hair – alopecia totalis, or hair loss involving the entire body – alopecia universalis
Alopecia Areata • Lifetime risk 1.7% • Associated with thyroid disease, vitiligo, inflammatory bowel disease • AA may be protective against the development of diabetes • Frequency of type I diabetes is increased in relatives of patients with alopecia areata
AA Histo • Lymphocytes surround lower portion of follicle in early lesions = “swarm of bees” • Increased numbers of miniature telogen and catagen follicles or sometimes early anagen hair follicles in the superficial dermis
Telogen effluvium • Early and excessive loss of normal club hairs from normal resting follicles in the scalp • Loss results from traumatization of the normal hair by some stimulus, such as surgery, parturition, fever, drugs, or traction which precipitates the anagen phase into catagen and telogen phases • Associated with Fe deficiency and thyroid disease • Follicle is not diseased and inflammation is absent
Telogen effluvium • “lots of hairs coming out by the roots” • Loss is diffuse and only infrequently causes clinically perceptible thinning of hair • Normal telogen count is below 10% • Can be estimated by the pull test • Grasping 40 hairs firmly between thumb and forefinger, followed by a slow pull • Greater than 4-6 club hairs is abnormal
A Telogen fibers showing a club shape • B Anagen fibers with attached inner root sheath, demonstrating pigmented, distorted bulbs appearing like the end of a broomstick
Telogen effluvium • 100 – 200 hairs lost daily • 200 – 400 lost in telogen effluvium
TX • No specific therapy • In the majority of cases it will stop spontaneously within a few months and the hair will regrow • Chronic form may occur • 5% minoxidil solution • education
Anagen effluvium • Seen frequently following the administration of cancer chemotherapeutic agents, such as antimetabolites, alkylating agents, and mitotic inhibitors • Only anagen hairs are involved • With cessation of the drug the follicle resumes normal activity within a few weeks • Process entirely reversible • Topical minoxidil may decrease the period of baldness by an average of 50 days
Androgenetic alopeciamale-pattern baldness • Most prevalent type of hair loss in humans • Can be inherited from either or both parents • Starts during the 20s to early 30s by gradual loss of hair, chiefly from the vertex and frontotemporal regions • Several patterns • Rate varies
Pathogenesis of AGA • Related to dihydrotestosterone (DHT) • Testosterone converted to DHT by 5alpha – reductase • Two isoenzymes, type I and type II • Type I 5alpha – reductase predominantly found in sebaceous glands and the liver as well as scalp hair follicles • Type II 5alpha – reductase is present in scalp hair follicles, beard, and chest hair, liver, and prostate • Genetic absence of type II 5alpha – reductase is protective from the development of male AGA
AGA TX • Minoxidil • 2% and 5% • Indefinite treatment to maintain a response • 1/3 cases grow cosmetically useful hair • Finasteride • Effective in preventing further hair loss (90% of men) and in increasing the hair counts (65% of men) • Hair transplantation
Androgenetic alopecia in women • Generally diffuse hair loss throughout the midscalp, sparing the frontal hairline except for slight recession • The midline part is an important clinical clue to the diagnosis, revealing this central thinning by the appearance of the “Christmas tree pattern” • The cause is now believed to be a genetic predisposition in combination with an excessive androgen response
TX • Topical minoxidil 2% • Spironolactone or finasteride if associated with hyperandrogenemia
Trichotillomania • A neurotic practice of plucking or breaking hair from the scalp, eyelashes, eyebrows, extremities, or pubic region • Usually localized but may be widespread • Areas of alopecia characteristically contain hairs of various lengths • Seen mostly in girls under 10 and women, may also be seen in boys and adults
Trichotillomania • It has been suggested that one ask the child not if but rather how the removal is done • Shave 3 X 3 cm area and watch the hair regrow normally. Hairs in this “skin window” will be too short for plucking • Biopsy – high number of catagen hairs, pigmentary defects and casts, trichomalacia and hemorrhage, follicular plugging
May be a manifestation of obsessive-compulsive disorder May be assoc with depression or anxiety TX – psychotherapy, behavioral therapy or an appropriate psychopharmacologic medication fluoxetine Trichotillomania
Traction alopecia • Occurs from prolonged tension on the hair • Either from the hair tightly braided or in a ponytail
Hot comb alopecia • Develops characteristically on the crown and spreads peripherally to form a large oval area of partial hair loss • Initially reported in black women who straightened their hair with hot combs • The hot petrolatum used with the iron causes thermal damage to the hair follicle • Histo same as for trichotillomania and traction alopecia (follicular degeneration syndrome
Follicular degeneration syndrome • Pigmented casts in follicle • Empty follicles • Perifollicular lymphocytes, plasma cells, or neutrophils usually sparse or absent • Perifollicular hemorrhage sometimes • Perifollicular fibrosis if follicle is destroyed
Alopecia syphilitica • May have a typical moth-eaten appearance on the occipital scalp, a generalized thinning, or a combination of the two • Eyebrows and lashes, and other body hair may be involved • May be the first sign of a syphilis infection
Tumor alopecia • Refers to hair loss in the immediate vicinity of either benign or malignant tumors of the scalp • Syringomas, nerve sheath myxomas, and steatocytoma multiplex • Alopecia neoplastica – hair loss from metastatic tumors, most commonly breast carcinoma
Pseudopelade of Brocq • Non-inflammatory, intermittently progressive scarring alopecia • Unknown origin • Lesions typically start on the crown and spread in a “pseudopod-like” fashion at irregular intervals • Clinically, pale depressed areas called “footprints in the snow” • Histo: development of elastic fibers around the lower part of the follicle and less perifollicular inflammation • Tx: difficult; surgery best option
Follicular mucinosis(alopecia mucinosa) • Most commonly occurs on the scalp or beard area • Cicatricial alopecia occurs when enough mucin is deposited in the follicular outer root sheath and sebaceous gland to cause extensive follicular disruption • Otherwise alopecia may be reversible • Primary cases occur either as localized lesions of the head or neck typically resloving within a year
Follicular mucinosis(alopecia mucinosa) • More generalized lesion have a longer course • Young people are primarily affected • A secondary type – associated with cutaneous T-cell lymphoma, usually more widespread and in older persons
Inflammatory alopecia • May be seen in lichen simplex chronicus and various eczematous changes on the scalp, including kerion • DLE, lichen planopilaris, sarcoidosis, and folliculitis decalvans are the commonest inflammatory causes of cicatricial alopecia
Increased fragility Trichothiodystrophy Pili torti Monilethrix Trichorrhexis nodosa Trichorrhexis invaginata No increased fragility Loose anagen hair syndrome Uncombable hair Woolly hair Pili multigemini Pili annulati Pili bifurcati HAIR STRUCTURE DEFECTS
Hair structure defects Increased fragility
Autosomal recessive Brittle hair with markedly reduced sulfur content Sulfur reduced 50% of normal value Distinctive features under polarized light and scanning electron microscopy Trichothiodystrophy
With light microscopy trichoschisis (clean transverse fractures) may be seen With polarized microscopy the hair shows alternating bright and dark regions Trichothiodystrophy