ECG interpretation for beginners Part 3 - Bradyarrhythmias
560 likes | 2.76k Vues
ECG interpretation for beginners Part 3 - Bradyarrhythmias. Paul Williams Cardiology Specialist Registrar. Normal ECG!. Native pacemaker sites. SA node SR (50-180) Escape rhythms AV node “junctional” - narrow 50-60bpm Ventricle “ventricular” - broad 30-40bpm Unstable.

ECG interpretation for beginners Part 3 - Bradyarrhythmias
E N D
Presentation Transcript
ECG interpretation for beginnersPart 3 - Bradyarrhythmias Paul Williams Cardiology Specialist Registrar
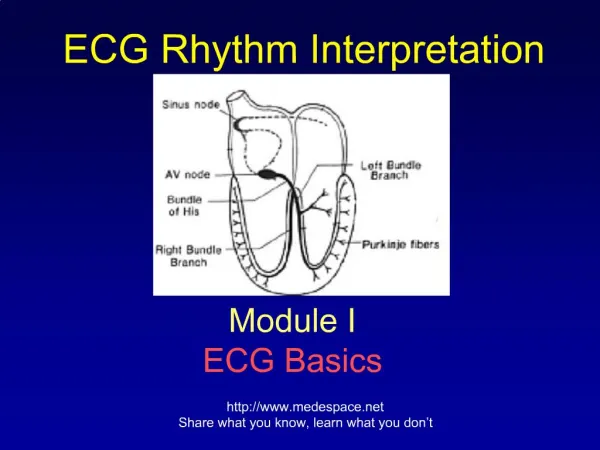
Native pacemaker sites • SA node • SR (50-180) • Escape rhythms • AV node • “junctional” - narrow • 50-60bpm • Ventricle • “ventricular” - broad • 30-40bpm • Unstable
Only two things make your heart go too slow! 1) Failure of normal pacemaker 2) Blocked conduction at the AV node DANGEROUS!
Is it a problem with the SA node or the AV node (or both)? • Sinus bradycardia • SA nodal disease • Junctional rhythm (escape) • AV block • 1 HB (doesn’t affect rate) • 2 HB – Wenckebach (doesn’t need PPM). Mobitz type 2 • 3 HB (or CHB) • Slow AF
Key questions Concentrate on rhythm strip (II, V1) • Are there P waves at all? • Is there a P wave before each QRS? Use a piece of paper if not sure For management Is this causing symptoms? Is this dangerous? Is there a risk of asystole?
Sinus bradycardia • Normal • No treatment!
AV block • All indicate problems with AV nodal conduction • 3 degrees - progressive • Usually intermittent to start with • Higher degree AV block is dangerous and needs a PPM (risk of asystole & VF) • Most rate-lowering drugs work by slowing AV conduction
AV block – 1st degree • Lengthened PR interval (>0.2s) • Always P wave before each QRS • Doesn’t affect rate so not necessarily bradycardic…. • In isolation doesn’t need treatment
AV block – 2nd degree Two types: • Mobitz one • Wenckebach phenomenon • Usually benign if sleeping • Mobitz two • 2:1, 3:1, 4:1 etc • Not benign!!! • Risk of SCD - needs a PPM
Wenckebach • Karel Frederik Wenckebach • Dutch anatomist • 1864-1940
Complete heart block • Can only reliably be diagnosed if patient in SR (so can see P waves) • No relationship between P waves & QRS complexes. Usually both will be regular • Is there a risk of imminent asystole? • Very slow rate • Pauses • Broad QRS (ie. ventricular escape rhythm) • Needs a PPM if occurs off drugs • Needs a TPW if symptomatic or high-risk features • Exception = transient CHB during inferior MI
Slow AF/flutter • Normally AF/flutter is fast! • AV conduction must be slowed • ? Drugs ? AV nodal disease • If ventricular rhythm is slow, regular and broad likely to be CHB with ventricular escape (easily missed)
Management of bradyarrhythmias • ABC! • Conscious? BP? CPR External pacing Temporary pacing wire Permanent pacemaker
External pacing • Most “defibs” can also pace • Must have limb leads on • Two main options: • Rate • Power • It is painful (sedation) & unreliable • Only stopgap measure
Temporary pacing wire • Need central access (jugular, femoral, subclavian) • Pass wire to heart using fluoroscopy • High complication rate in amateur hands • Not commonly performed now as external pacing available and little wait for PPMs
Further management • Stop bradycardic agents • B-blockers • Ca-blockers, • Digoxin • Amiodarone • Sotalol • Consider a PPM
Permanent pacemakers • Improve prognosis • 2nd degree and 3rd degree HB • Improve symptoms • SA nodal disease • Or both…..
Pacemaker types • One lead? (VVI) • RV • Two leads? (DDD) • RV and RA • Three leads? (BiV-PPM or CRT) • RV, RA and LV (via coronary sinus) • Any of above + defib (ICD)
Question 1 • What is the rate, rhythm and axis? • Management
Question 2 • What is the rate, rhythm and axis? • Management?
Question 3 • What is the rate, rhythm and axis? • Management?
Question 4 • What is the rate, rhythm and axis? • Management?
Question 5 • What is the rate & rhythm? • Management?