ECG Interpretation
ECG Interpretation. Supraventricular Tachycardia: Mechanisms, Diagnosis, & Management. William A. Shapiro, M.D. http://anesthesia.ucsf.edu/shapiro. advancing health worldwide TM. Department of Anesthesia and Perioperative Care . Normal Sinus Rhythm.

ECG Interpretation
E N D
Presentation Transcript
ECG Interpretation Supraventricular Tachycardia:Mechanisms, Diagnosis, & Management William A. Shapiro, M.D. http://anesthesia.ucsf.edu/shapiro advancing health worldwide TM Department of Anesthesia and Perioperative Care
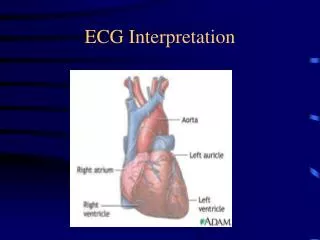
Normal Sinus Rhythm Normal sinus rhythm results from the initiation of an electrical signal (the cardiac impulse) by cells of the sinus node at a rate appropriate to the age and state of activity of the individual, and then the propagation of that signal in an orderly manner through the atria, A-V junction, ventricular specialized conducting system and the ventricular myocardium
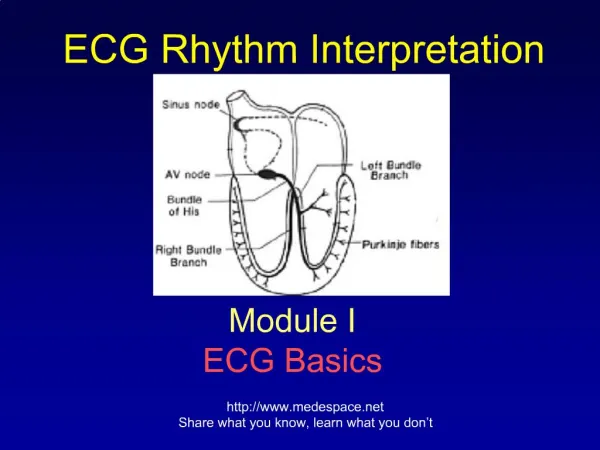
Cardiac Conduction System Bachmann’s bundle Sinus node Internodal pathways Left bundle branch AV node Posterior division Bundle of His Anterior division Purkinje fibers Right bundle branch
Arrhythmia An arrhythmia reflects either abnormally rapid or slow impulse initiation by the sinus node, or interruption of the sinus rhythm by impulses originating from some other site in the heart, either for short or long periods of time
Mechanisms of Arrhythmias • Reentry • Automaticity • Altered normal automaticity • Abnormal automaticity • Triggered Rhythms due to DAD (delayed after depolarizations
Causes of Arrhythmias • Physiologic and Pathologic Processes • Vagal stimulation, Fever, Hypothermia • Electrolyte abnormalities, CNS problems • Hypovolemia, Pain, anaphylaxis, etc. • Preexisting Cardiac & Pulmonary Disease • Acute coronary syndrome, HTN, AODM • COPD, hypoxia, hypercarbia
Supraventricular Tachycardia Definition • All forms of tachycardia (rate > 100 bpm) that arise above the bifurcation of the His bundle. Paroxysmal = sudden onset. • Require AVN or atrial tissue, or both, for initiation and maintenance of the arrhythmia. • Typically (P)SVT has a narrow QRS complex, but the QRS complex may be wide at baseline, or become wide due to rate dependent BBB. • Most reviews exclude A-fib & A-flutter, and MAT.
Supraventricular Tachycardia Incidence/Prevalence • Prevalence is distinct from incidence. • Prevalence is a measurement of all individuals affected by the disease within a particular period of time, whereas; • Incidence is a measurement of the number of new individuals who contract a disease during a particular period of time. Reference: http://en.wikipedia.org/wiki/Prevalence
Supraventricular Tachycardia Incidence/Prevalence • Incidence (new cases): 35 cases per 100,000 persons per year. • Prevalence (all affected): 2.25 per 1000 (excluding atrial fibrillation, atrial flutter, and multifocal atrial tachycardia). • Increases with age and the presence of CV disease. • Not usually associated with structural heart disease. Delacrétaz E. Supraventricular Tachycardia. N Engl J Med. 2006
Supraventricular Tachycardia Symptoms • Palpitations: A trigger is usually not identified. • Feeling of heart pounding in the chest and neck. • Anxiety, light-headedness, dyspnea. • Syncope and chest pain are uncommon, but may indicate CAD, especially in older patients. • Psychological stress is very common.
Supraventricular Tachycardia Mechanisms • Reentry- approx 90% of all SVT. Either reentry within the AVN (60%) or using an accessory bypass tract (30%). Almost all reentrant SVTs are started with a PAC. • Atrial focus- approx 10%. Automaticity or Triggered activity • Important concepts- conduction time and refractory period. • Fast conduction typically has a long refractory period. • Slow conduction typically has a sort refractory period.
Supraventricular Tachycardia Onset of SVT
Supraventricular Tachycardia Mechanisms Ferguson JD. Contemporary Management of Supraventricular Tachycardia. Circulation. 2003
What’s missing? Supraventricular Tachycardia Is this Sinus Rhythm or SVT?
Supraventricular Tachycardia What’s happening here?
Supraventricular Tachycardia Classification • AV Node Dependent- Reentry- approx 90% of all SVT. Either reentry within the AVN (60%) or using an accessory bypass tract (30%). • AV Node Independent- Atrial focus- approx 10%. Automaticity or Triggered activity. • Thinking of SVT in this way can help with treatment.
Treatment of All Cardiac Arrhythmias All arrhythmias that are hemodynamically significant require immediate cardioversion, defibrillation, or cardiac pacing
Supraventricular Tachycardia Treatment • AV Node Dependent- Vagotonic maneuvers- CSM, facial emersion in water, coughing, straining, etc. Drugs- Adenosine: 6 or 12 mg., verapamil: 5 mg up to 15 mg Diltiazem, beta blockers may also be used on the AVN. Ibutilide, procainamide, and flecainide, affect the bypass tract • AV Node Independent- Heart rate control is the goal. Beta Blockers- sotalol. • Catheter ablation considered a long term option.
Supraventricular Tachycardia Not Discussed • Atrial Fibrillation • Atrial Flutter • Multifocal Atrial Tachycardia • Sinus Node Arrhythmias
Supraventricular Tachycardia References • Fox DJ, et al. Supraventricular Tachycardia: Diagnosis and Management. Mayo Clin Proc. 2008;83(12):1400-11 • Delacrétaz E. Supraventricular Tachycardia.N Engl J Med. 2006;354:1039-51 • ACC/AHA/ESC guide-lines for the management of patients with supra- ventricular arrhythmias. J Am Coll Cardiol. 2003 Oct 15;42(8):1493-531 • Ferguson JD, et al. Contemporary Management of Paroxysmal Supraventricular Tachycardia.Circulation 2003;107:1096-1099 • Salerno JC, et al.Supraventricular Tachycardia.Arch Pediatr Adolesc Med. 2009;163(3):268-274