GASTROINTESTINAL BLEEDING
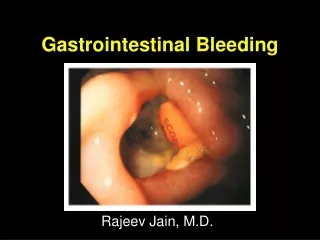
GASTROINTESTINAL BLEEDING. David A. Gremse, MD, FAAP, FACG Professor and Chair of Pediatrics University of Nevada School of Medicine. Gastrointestinal Bleeding. Hematemesis- Vomiting of bright red blood usually represents bleeding proximal to the ligament of Treitz

GASTROINTESTINAL BLEEDING
E N D
Presentation Transcript
GASTROINTESTINAL BLEEDING David A. Gremse, MD, FAAP, FACG Professor and Chair of Pediatrics University of Nevada School of Medicine
Gastrointestinal Bleeding • Hematemesis- Vomiting of bright red blood • usually represents bleeding proximal to the ligament of Treitz • Hematochezia- bright red blood per rectum • indicates a lower GI source of bleeding • Blood has a laxative effect so with massive bleeding the stool may be bright red
Gastrointestinal Bleeding • Blood streaks on the stool indicates anal outlet bleeding • Blood mixed with stool indicates bleeding source higher than the rectum • Blood with mucus indicates an infectious or inflammatory disease • Currant jelly-like material indicates vascular congestion and hyperemia (intussusception or midgut volvulus)
Gastrointestinal Bleeding • Maroon-colored stools indicate voluminous bleeding proximal to the rectosigmoid area • Melena, passage of black, sticky (tarry) stools suggests upper GI tract bleeding, but can be as distal as the right colon • Hematemesis suggests a large bleed with possible recurrence, melena alone indicates less voluminous bleeding
Common Nasopharyngeal bleeding Erosive Esophagitis Peptic ulcer Gastritis (H. pylori) Mallory-Weiss tear Prolapse gastropathy Less Common Bleeding disorders Duplication cyst Foreign body Tube trauma Vascular malformation Esophageal varices Causes of Upper GI Bleeding
Common Anal fissure Infectious colitis Salmonella, Shigella, Campylobacter, C.diff Inflammatory bowel disease Intussusception Upper GI source Less Common Meckel’s diverticulum Duplication cyst Hirschsprung’s enterocolitis Gangrenous intestine Vascular malformation Causes of Lower GI Bleeding
Clinical Findings in PUDNeonatal Period • Gastric ulcers are more common than duodenal ulcers in neonates • Spontaneous Perforation is a more common presentation than bleeding • Frequently associated with: • Hypoxia, Sepsis, RDS, CNS disorder
Clinical Findings in PUDInfants and Toddlers • Presenting symptoms: • Vomiting • Poor feeding • Irritability during and after eating • Abdominal distention • Hematemesis, melena • Commonly associated with underlying disease in this age group
Clinical Findings in PUDPre-Schoolers • Periumbilical or generalized abdominal pain • Vomiting after eating • Nocturnal or early morning pain • Gastric ulcers are as common as duodenal ulcers • Primary ulcers are as common as secondary ulcers
Clinical Findings in PUDSchool Age • Male: Female ratio is 3:1 • Burning epigastric pain • Nocturnal pain • Melena, hematemesis, fecal occult blood • Primary ulcers are more common than secondary ulcers
Pathophysiology of GI Bleeding • Mucosal lesions • Acid-peptic disease, drug-induced (NSAIDs), Infectious (H. pylori), inflammatory bowel dz • Portal hypertension • Esophageal varices, hypertensive gastropathy • Coagulopathy - Hemophilia, hepatic coagulopathy, CHF w/hepatic congestion • Vascular lesions - hemangiomas
Causes and Effects of H+ Ion Backdiffusion Lowflow states Drugs, EtOH Stress H. pylori Bile Reflux Mucosal Barrier Break H+ Parietal Cells Release of histamine + Vasodilatation Increased HCl and Pepsin Secretion
Peptic Ulcer DiseaseDiagnostic Evaluation • History (medications, family history) • Physical exam (include Hemoccult) • CBC, type & screen for GI bleeding • PT, PTT • H. pylori antibody, fasting gastrin level • Upper GI Series • EGD
Indications for EGD • Hematemesis, Melena, Heme (+) stool • Severe pain, weight loss • Unexplained anemia • Symptoms persist despite trial of antisecretory therapy • Evaluation of abnormal UGI series • Evaluation of status of H. pylori
Case #1 – UGI Bleeding • 12 YOWF with S/P splenectomy 2 yr ago for Evan’s syndrome • Weakness, pallor, melana x 2 days • Exam – HR- 128, BP-86/54, tachycardic, pale, abdomen nontender, nondistended, no hepatomegaly • Lab – H/H=6.8/19.1, WBC, 5.7; platelets, 115,000, PT=13.2 sec; AST, 38; ALT, 45; T.bili, 0.5; alk phos, 227
Case #2 – UGI Bleeding • 11 YOWM previously healthy with 1 day h/o fever, vomiting and diarrhea • Emesis x 6 over past 24 hr, w/blood last 2 times • Exam – HR- 84, BP-116/74, abdomen nontender, nondistended, no hepatomegaly • Lab – H/H=13.8/39.1, WBC, 8.7; platelets, 235,000, PT=12.2 sec
Meckel’s Scan • 99mTc-Pertechnetate Scan - injected IV and accumulates in gastric tissue - RLQ uptake is diagnostic of Meckel’s diverticulum • False (+) - bleeding lesions such as Crohn’s disease, intussusception, hemangioma, PUD • False (-) - Barium, bladder overdistention, no gastric mucosa in diverticulum
99mTc- Labeled Red Cell Scan • 99mTc-sulfur colloid is added to a sample of the patient’s blood cells and re-infused IV- patient is scanned with gamma camera • Half-life is short (2.5 min) so that after 10 minutes only 10% is left in the circulation • 99mTc accumulates at the bleeding site and lights up on scan - can detect 0.1 ml/min
GI Bleeding - Treatment • ABCs - protect airway with hematemesis in an obtunded patient • IV access - two lines (0.9% NS in one line, PRBC’s not compatible with dextrose) • Transfuse for Hgb < 8 w/active bleeding • NG lavage • Antacids (1 ml/kg up to 30 ml q 2 hr) • PPI 2 mg/kg loading dose, then 1 mg/kg/day IV
Drug Efficacy in Healing Ulcers • DrugRegimenUlcers Healed • H2RA4 weeks 8 weeks • Cimetidine 40 mg/k/d 80% 90% • Ranitidine 4-8 mg/k/d • Famotidine 1-2 mg/k/d • PPIs • Omeprazole 0.7-3 mg/k/d 85% 95% • Lansoprazole 0.7-4 mg/k/d • Sucralfate 40-80 mg/k/d 75% 86%
Management • Class 1, no anemia, no active bleeding on lavage, may be followed up as outpatient • Class 2, mild anemia, active bleeding may be monitored on wards • Class 3 or 4 admit to PICU, central line, arterial line • IVF boluses, transfusion as needed
Management • Iced saline? - with cooling, bleeding time increases to 3 x control, clotting time increases up to 60%, and PT can increase to 2 x control, and can cause hypothermia • NG tube is useful to monitor bleeding, but not in treatment • Therapeutic endoscopy (sclerotherapy) useful in variceal hemorrhage
Management - Octreotide • Somatostatin analog - octreotide has a longer half-life than somatostatin • Decreases splanchnic blood flow and gastrointestinal secretion • Make a 1 g/ml drip - begin drip at a rate of 0.1 g/kg/min - increase to 0.5 g/kg/min until bleeding stops, then wean rate • Side effects - nausea, gas, hyperglycemia, gallstones, elevated liver enzymes
GI Bleeding – Summary • Remember your abC’s • IV access if bleeding is significant • Plan diagnostic work-up based on presentation • Consider non-GI causes of blood in the GI tract (e.g., swallowed blood)
Question #1 • An 18-month-old boy passed a dark red stool four hours ago and another bloody stool during physical examination. He has no fever, vomiting, diarrhea, or constipation. His growth and development have been normal. On physical examination, his pulse is 140/min, respiratory rate 24/min, and blood pressure is 86/54 mmHg. The abdomen is soft and nontender. Rectal examination reveals maroon-colored stool that is guaiac positive. The remainder of the physical examination is normal. Gastric aspirate is negative for blood. Laboratory evaluation reveals hemoglobin 8 g/dL, hematocrit 26%. Prothrombin time, partial thromboplastin time, and INR were normal. After intravenous fluid administration and erythrocyte transfusion, which of the following is most likely to be diagnostic? A. Barium enema B. Meckel radionuclide scan C. Computerized tomography (CT scan) of the abdomen D. Upper gastrointestinal series with small bowel follow through E. Abdominal angiography
Question #2 • A 6-week-old infant has done well since birth until blood and mucus appeared in the stool for the past 3 days. He is taking his usual four ounces of cow-milk formula per feeding without vomiting. He is more irritable during defecation. Physical examination reveals that the abdomen is soft and not distended. The hemoglobin is 10 g/dL. • Which of the following is the most likely explanation for the findings in this infant? A. Hirschsprung disease B. Meckel diverticulum C. Anal fissure D. Cow-milk protein colitis E. Midgut volvulus