Acute Gastrointestinal Bleeding
Acute Gastrointestinal Bleeding. Rajeev Jain, M.D. GI Bleeding. Clinical Presentation Acute Upper GI Bleed Acute Lower GI Bleed . Case Presentation. CC: Melena HPI: 54 yo man taking ibuprofen 200 mg po tid for the past 2 wks b/o acute LBP after lifting presents with 2 day h/o melena

Acute Gastrointestinal Bleeding
E N D
Presentation Transcript
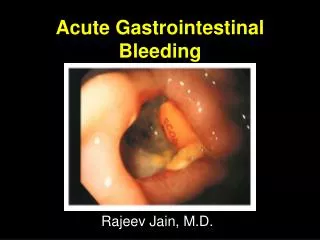
Acute Gastrointestinal Bleeding Rajeev Jain, M.D.
GI Bleeding • Clinical Presentation • Acute Upper GI Bleed • Acute Lower GI Bleed
Case Presentation • CC: Melena • HPI: 54 yo man taking ibuprofen 200 mg po tid for the past 2 wks b/o acute LBP after lifting presents with 2 day h/o melena • PMHx: neg All: NKDA SHx/FHx: neg • Vitals: BP 105/75 P 90 • PE: normal
Clinical Presentation Hematemesis: bloody vomitus (bright red or coffee-grounds) Melena: black, tarry, foul-smelling stool Hematochezia: bright red or maroon blood per rectum Occult: positive guaiac test Symptoms of anemia: angina, dyspnea, or lightheadedness
Patient Assessment • Hemodynamic status • Localization of bleeding source • CBC, PT, and T & C • Risk factors • Prior h/o PUD or bleeding • Cirrhosis • Coagulopathy • ASA or NSAID’s
Resuscitation • 2 large bore peripheral IV’s • Normal saline or LR • Packed RBCs • Correct coagulopathy
Location of Bleeding • Upper • Proximal to Ligament of Treitz • Melena (100-200 cc of blood) • Azotemia • Nasogatric aspirate • Lower • Distal to Ligament of Treitz • Hematochezia
Acute UGIBDemographics • 10,000 - 20,000 deaths annually • Mortality stable at 10% • 80% self-limited • Continued or recurrent bleeding - mortality 30-40%
Acute UGIBPrognostic Indicators • Cause of bleeding • Severity of initial bleed • Age of the patient • Comorbid conditions • Onset of bleeding during hospitalization
Acute UGIBPrognostic Indicators Tedesco et al. ASGE Bleeding Survey. Gastro Endo. 1981.
Peptic ulcer disease Gastric ulcer Duodenal ulcer Mallory-Weiss tear Portal hypertension Esophagogastric varices Gastropathy Esophagitis Dieulafoy’s lesion Vascular anomalies Hemobilia Hemorrhagic gastropathy Aortoenteric fistula Neoplasms Gastric cancer Kaposi’s sarcoma Acute UGIBDifferential Diagnosis
Acute UGIBFinal Diagnoses of the Cause in 2225 Patients Tedesco et al. ASGE Bleeding Survey. Gastro Endo. 1981.
Acute UGIBCauses in CURE Hemostasis Studies (n=948) Savides et al. Endoscopy 1996;28:244-8.
Acute UGIB CORI Database University, VA, & private practices 20 months (12/99-7/01) 7822 EGDs for UGIB BoonpongmaneeS. et al. Gastrointest Endosc 2004;59:788-94.
Prognostic Features at Endoscopy in Acute Ulcer Bleeding Laine and Peterson New Eng J Med 1994;331:717-27.
Thermal Bipolar probe Monopolar probe Argon plasma coagulator Heater probe Mechanical Hemoclips Band ligation Injection Epinephrine Alcohol Ethanolamine Polidocal Endoscopic Therapy of PUD
Endoscopic Therapy of PUD Laine and Peterson New Eng J Med 1994;331:717-27.
Adjuvant Medical Therapy of PUD • Acid suppression (intragastric pH > 4) • Histamine 2 Receptor Antagonists (H2RAs) • Ranitidine (Zantac) • Famotidine (Pepcid) • Proton Pump Inhibitors (PPIs) • Pantoprazole (Protonix) • Lansoprazole (Prevacid) • Esomeprazole (Nexium)
Duodenal ulcer: no benefit Gastric ulcer: mild benefit Mortality ARR 3%; NNT 33 Surgery ARR 7%; NNT 14 Rebleeding ARR 7%; NNT 14 Caveats Tolerance develops within 24 hrs More potent acid suppression available Bleeding PUD: IV H2RAsMeta-Analysis Levine JE et al. Aliment Pharmacol Ther 2002;16:1137-42.
Adjuvant Medical Therapy of PUD 739 patients admitted with GI bleeding 472 patients required no endoscopic treatment 267 received endoscopic treatment 27 patients not included: comorbid or no consent 120 patients received IV omeprazole 80 mg bolus then 8 mg/hr for 72 hours 120 patients received placebo Lau et al. New Eng J Med 2000;343:310-316.
Adjuvant Medical Therapy of PUD Lau et al. New Eng J Med 2000;343:310-316.
Bleeding PUD: PO/IV PPIsMeta-Analysis • Reduction in: • Rebleeding NNT* 4-17 • Surgery NNT* 6-25 • No change in mortality • PPIs add to endoscopic therapy but do not supplant endoscopic therapy * Estimates from pooled ORs Leontiadis, GI et al. BMJ 2005;330:568-75.
MEDICAL THERAPYAcute Variceal Bleeding • Vasopressin/Glypressin • Nonselective vasoconstrictor • 50% efficacy in controlling bleeding • 25% vasospastic side effects • Octreotide • Cyclic octapeptide analog of somatostatin • Longer acting than somatostatin • Equivalent to sclerotherapy and improves endoscopic results
TIPS Coronary Vein IVC Splenic Vein Portal Vein
Aortoduodenal Fistula Aorta Duodenum Fistula Graft
Acute BleedingChanges Before and After 2 Liter Bleed 45% 45% 27%
Acute UGIBSurgery • Recurrent bleeding despite endoscopic therapy • > 6-8 units pRBCs
Case Presentation • CC: Hematochezia • HPI: 74 yo woman presents with 6 hour history of painless maroon blood per rectum • PMHx: CAD, Chol, AFib, CABG, L-CEA • Meds: ASA, coumadin, digoxin, lovastatin • Vitals: BP 105/75 P 90 • PE: irreg rhythm, maroon blood on DRE
Diverticulosis Colitis IBD (UC>>CD) Ischemia Infection Vascular anomalies Neoplasia Anorectal Hemorrhoids Fissure Dieulafoy’s lesion Varices Small bowel Rectal Aortoenteric fistula Kaposi’s sarcoma UPPER GI BLEED Acute LGIBDifferential Diagnosis
Acute LGIBDiagnoses in pts with hemodynamic compromise. Zuccaro. ASGE Clinical Update. 1999.
Urgent Colonoscopy for the Diagnosis and Treatment of Severe Diverticular Hemorrhage • 121 pts with severe bleeding (>4 hrs after hospitalization) • 1st 73 pts: no colonoscopic tx • Last 48 pts eligible for colonoscopic tx • Colonoscopy w/in 6-12 hrs
Urgent Colonoscopy for the Diagnosis and Treatment of Severe Diverticular Hemorrhage Jensen DM, et al. New Eng J Med 2000:342:78-82.
Acute LGIBMeckel’s Diverticulum • Incidence 0.3 - 3.0 % • Etiology Incomplete obliteration of the vitelline duct. • Pathology 50% ileal, 50% gastric, pancreatic, colonic mucosa • Complications • Painless bleeding (children, currant jelly) • Intussusception
Acute LGIBEvaluation Zuccaro. ASGE Clinical Update. 1999.
Acute LGIBKey Points • Resuscitation • UGI source • Most bleeding ceases • Colonscopy - early • No role for barium studies • 5% Mortality