Download
1 / 23
230 likes | 399 Vues
Pleural Effusions Internal Medicine AM Report Andrew Smitherman Wednesday May 27, 2009. Definition. Excess fluid in space between the lung and chest wall. Pathophysiology.

E N D
Pleural Effusions Internal Medicine AM Report Andrew Smitherman Wednesday May 27, 2009
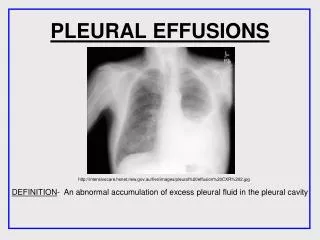
Definition Excess fluid in space between the lung and chest wall.
Pathophysiology • Fluid typically enters pleural space from capillaries in the parietal pleura, from the pulmonary interstitium via visceral pleura or from peritoneal cavity via small holes in the diaphragm. • Lymphatics are able to increase absorption 20 times that of normal if needed. • An effusion forms when the production of pleural fluid overwhelms the ability of the lymphatics to drain or due to decreased lymphatic drainage.
Etiologies Light, RW. Pleural Effusion. NEJM. 2002; 246: 1971-1977.
Initial Evaluation with Physical Exam Typical findings: Dullness to percussion, absence of tactile fremitus Diminished or absence of breath sounds Findings suggestive of a particular etiology: S3, Distended Neck Veins, Peripheral Edema – CHF RV Heave or Thrombophlebitis – Pulmonary Embolism Lymphadenopathy or Hepatosplenomegaly – Malignancy Ascities – Hepatic Failure / Cirrhosis
What’s My Claim to Fame? Josef Leopold Auenbrugger (1722 – 1809)
What’s My Claim to Fame? Josef Leopold Auenbrugger (1722 – 1809) Developed physical exam techniques of chest percussion and tactile fremitus
Indications for Thoracentesis • Diagnostic: effusion > 10mm in height on lateral decubitus or ultrasonography • Therapeutic: patient symptomatic – dyspnea at rest, increased O2 requirement. Removal of up to 1500mL indicated. • If patient presents with likely CHF exacerbation, with bilateral effusions, afebrile and reports no chest pain a trial of diuresis is reasonable and safe. • Greater than 80% of effusions due to CHF are bilateral • 75% of effusions due to CHF resolve in 48 hours of diuresis • If effusions persist for >72hrs a thoracentesis is indicated • Unilateral or Asymmetric effusions should be tapped Shinto RA and Light RW. Effects of Diuresis on the Characteristics of Pleural Fluid in Patients with Congestive Heart Failure. American Journal of Medicine. 1990; 88: 230-234.
Do I Need a Follow-up Chest Radiograph? • Not needed unless air is obtained during procedure; coughing, chest pain or dyspnea develops; or tactile fremitus is lost over apex of aspirated hemithorax. • Of 506 thoracenteses, pneumothorax found in 13 of 18 (72%) with one or more of the above findings but only in 5 of 488 (1%) with none of the above. Aleman C, Alegre J, Armadans L. The Value of the Chest Roentgenography in the Diagnosis of Pneumothorax After Thoracentesis. American Journal of Medicine. 1999; 107: 340-343.
Transudate v. Exudate • Transudate: usually due to systemic changes and an imbalance between hydrostatic and oncotic forces. • CHF, Cirrhosis, Pulmonary Embolism • Exudate: due to local changes that lead to fluid accumulation. • Pneumonia, Malignancy, Pulmonary Embolism
Transudate v. Exudate • By the Light’s Criteria alone, 17 of 100 samples tested will falsely be categorized as an exudate. • If you have a clinical situation where transudate seems more plausible, compare pleural fluid and serum albumin. If Alb(serum) – Alb(PF) > 1.2 g/dL a transudative process is more likely. • An albumin difference of ≤ 1.2g/dL will incorrectly identify an effusion as exudative in 8% of cases.
Cell Count and Differential • Neutrophilic: • Seen when acute process is involving pleura • Parapneumonic, PE, Pancreatitis • Lymphocytic • Malignancy or Tuberculosis
Glucose • Low glucose (<60mg/dL) in pleural fluid is an indication of: • Parapneumonic or Malignant Effusion • Less commonly hemothorax, Tuberculosis, rheumatoid pleuritis
LDH • Correlates to degree of pleural inflammation. • An increasing LDH level on subsequent thoracenteses is suggestive of worsening inflammation.
Cytology and Malignant Effusions • 75% of malignant effusions are associated with lung carcinoma, breast carcinoma or lymphoma. • Reported sensitivity of cytology for diagnosing the following: • Lymphoma (25-50%) • Sarcoma Involving Pleura (25%) • Squamous Cell Carcinoma (20%) • Mesothelioma (10%) Light, RW. Pleural Effusion. NEJM. 2002; 246: 1971-1977.
Parapneumonic • Features of pleural effusion that is suggestive of needing more invasive procedure than thoracentesis: • Loculated Pleural Fluid • Pleural Fluid pH < 7.2 • Pleural Fluid Glucose < 60mg/dL • Positive Gram Stain or Culture • Gross pus in Pleural Space
Tuberculous Pleuritis • Suspected based on History and a lymphocytic predominance on cell differentiation. • Less than 40% of tuberculous effusions will have positive pleural-fluid culture. • Adenosine Deaminase is sensitive (99.6%) and specific (97.1%) when a cut-off of 40U/L is used. Lee YCG, Rogers JT, Rodriguez RM, Miller KD and Light RW. Adenosine Deaminase Levels in Nontuberculous Lymphocytic Pleural Effusions. Chest 2001; 120: 356-361.
Miscellaneous Pearls • Elevated Amylase: suggestive of esophageal rupture or pancreatic disease • Eosinophilia: associated with Drug-Induced Effusions • Fever, PMN predominance, no lung parenchymal lesion – intraabdominal abscess
References • Aleman C, Alegre J, Armadans L. The Value of the Chest Roentgenography in the Diagnosis of Pneumothorax After Thoracentesis. American Journal of Medicine. 1999; 107: 340-343. • Kasper DL, Braunwald E, Fauci AS, Hauser SL, Longo DL, Jameson LJ eds. Harrison’s Principles of Internal Medicine. 16th ed. New York: McGraw-Hill, 2005. • Lee YCG, Rogers JT, Rodriguez RM, Miller KD and Light RW. Adenosine Deaminase Levels in Nontuberculous Lymphocytic Pleural Effusions. Chest 2001; 120: 356-361. • Light, RW. Pleural Effusion. NEJM. 2002; 246: 1971-1977. • Shinto RA and Light RW. Effects of Diuresis on the Characteristics of Pleural Fluid in Patients with Congestive Heart Failure. American Journal of Medicine. 1990; 88: 230-234.