Download
1 / 16
210 likes | 1.87k Vues
Venous Blood Gas Versus Arterial Blood Gas Analysis. Ping-Wei Chen PGY-2 Emergency Medicine. It’s Go Time…. 25 yo female Single vehicle rollover near Sundre Intubated for deteriorating GCS In the ED: BP 70 palp, HR 122 Not responding to painful stimuli

E N D
Venous Blood Gas VersusArterial Blood GasAnalysis Ping-Wei Chen PGY-2 Emergency Medicine
It’s Go Time… • 25 yo female • Single vehicle rollover near Sundre • Intubated for deteriorating GCS • In the ED: • BP 70 palp, HR 122 • Not responding to painful stimuli • 01:23 - VBG ordered as part of workup • 01:41 – ABG ordered as part of workup
Objectives • Controversy • Can VBGs replace ABGs? • When are VBGs and ABGs different? • When might I want an ABG? • NOT covered • Electrolytes • Lactate
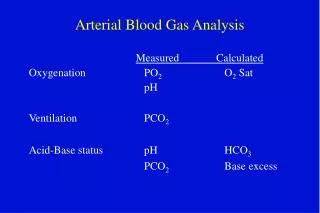
What’s all the fuss about? Arterial Blood Gas Venous Blood Gas Samples can be drawn simultaneously at time of venipuncture Should be done without tourniquette More difficult to obtain in pulseless patients Controversy regarding level of agreement with arterial values • PAINFUL • Arterial injury • Thrombosis with distal ischemia • Hemorrhage/hematoma • Aneurysm formation • Median nerve damage • Infection • Needlestick injury • Reflex sympathetic dystrophy
Prospective, observational study • 218 subjects, ED population • dyspnea, DKA, renal failure, seizures, ↓LOC, ingestions, ischemic colitis • A priori definition of clinically important difference • Pearson correlation coefficient • Bland-Altman plots Rang et al. 2002. Can J Emerg Med 4(1):7
Results • Excellent correlation • pH (r= 0.913) • pCO2 (r=0.921) • calculated HCO3 (r=0.953)
Results • Clinically Important Differences • 26/45 physicians responded
Result • Mean Differences • pH 0.036 (0.030-0.042) • pCO2 6.0 mm Hg (5.0-7.0) • HCO3 1.5 mEq/L (1.3-1.7)
Prospective, observational study • 246 subjects, ED population • acute respiratory disease, suspected metabolic disorder • pH only • Results: • Excellent correlation r=0.92 • Mean difference: 0.04 pH units (-0.11 to +0.04) Kelly et al. 2001. Emerg Med J. 18:340
Prospective, observational study • 95 patients, ED population • AECOPD, pneumonia, sepsis, ARF/CRF, DKA, ACS, acute gastroenteritis, SLE, toxic ingestion • Bland-Altman Analysis • Results: ABG compared to VBG
Review article: 6 studies • pH and HCO3 • Results: • Mean difference • pH: 0.02 (-0.009 to 0.021), n=258, DKA patients only • pH: 0.037 (-0.11 to 0.04), n =763, respiratory/metabolic illness • HCO3: -1.88 mEq/L (N/A), n =21, DKA patients only • HCO3: -0.99 mEq/L (-2.73 to 5.13), n=763, respiratory/metabolic illness
When are they different? • Weil et al. 1986. Difference in acid-base state between venous and arterial blood during cardiopulmonary resuscitation. NJEM. 315:153-6. • Prospective, observational study (n=16) • ICU/CCU patients • Arteriovenous gradient
So when might I want an ABG? • Unable to establish IV access • Inability to obtain sample • Inability to obtain O2 saturation by pulse oximeter • Peripheral vasoconstriction • Abnormal hemoglobins • Carboxyhemoglobin • Methemoglobin • Sickle hemoglobin
N = 1 • VBG at 01:32 • pH 7.11/pCO2 41/HCO3 14/lactate 6.6 • ABG at 01:41 • pH 7.12/pCO2 34/HCO3 11/lactate 6.1
Conclusions • VBGs not interchangeable with ABGs BUT • Excellent correlation with ABG values • Reasonable agreement on VBG for clinical decision making in ED • pH 0.02-0.04 lower • PCO2 3-6 mmHg higher • HCO3 essentially the same • Consider ABG in: • Inability to obtain sample • Inability to utilize pulse oximeter