Understanding Urinary Tract Infections: Pathophysiology, Diagnosis, and Management
200 likes | 405 Vues
Explore the pathophysiology of UTI, risk factors, common uropathogens, specimen collection techniques, and interpretation of urine culture results. Learn about different types of UTIs and their treatment options.

Understanding Urinary Tract Infections: Pathophysiology, Diagnosis, and Management
E N D
Presentation Transcript
Pathophysiology of urinary tract infection • Ascending route of infection is the most common. • Hospital infection associated with lower urinary tract instrumentation (catheterization, cystoscopy). • Once in the bladder uropathogens multiply, then pass up the ureters to the renal pelvis and parenchyma • Source of uropathogens: enteric bacteria mainly
Urinary tract infection more common in women than men • Short female urethra. • Close proximity to perianal areas. • Men also have an antibacterial substance in their prostate gland that reduces their risk.
Pathophysiology of urinary tract infection • Cystitis: (lower urinary tract infection) • Pyelonephritis: infection of the kidney • with acute suppurative inflammation of the • pelvis, • medullary and cortical tubules, • corticomedullary intersititum • Urosepsis: bacteremia due to pyelonephritis • Papillary necrosis • Sloughing of necrotic pyramids • Perinephric abscess
Risk factors in complicated urinary tract infection • Indwelling catheters • Urinary calculi • Neurogenic bladder • Prostatic enlargement • Uterine prolapse • Urologic instrumentation or surgery • Renal transplantation • Diabetes mellitus
Common uropathogens • Escherichia coli • Other Enterobacteriaceae (Klebsiella, Enterobacter, Proteus, Citrobacter) • Pseudomonas aeruginosa • Enterococcus • Staphylococcus saprophyticus • Staphylococcus aureus • Associated with staphylococcemia • Streptococcus agalactiae (group B) • Denotes vaginal colonization in pregnant women • Candida
Uncommon uropathogens • Corynebacterium urealyticum • Haemophilus influenzae and H. parainfluenzae • Blastomyces dermatitidis • Neisseria gonorrhaeae • Mycobacterium tuberculosis
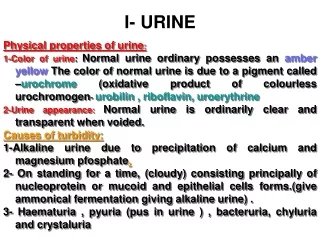
Notes • Adult urine volume = 600 – 2500 ml /24hr. • Oligouria: marked decrease in urine flow < 400 ml/24hr. • Polyuria: Marked increase in urine flow > 2500 ml/24hr. • Anuria: less than 100 ml/24hr. • Nocturia: excessive urination during night.
Aim of the test • An etiological diagnosis of bacterial urinary tract infection by quantitative • Cultivation of the urine with identification and susceptibility test of the isolated bacteria(s). • Criteria of specimen rejection • Un-refrigerated specimen older than 2 hours may be subject to overgrowth • unlabeled specimen; mislabeled specimen; • Specimen in expired transport container
Types of urine specimens • First-voided morning urine optimal (generally bacteria have been proliferating in bladder urine for several hours) • Midstream urine specimens (initially voided urine contains urethral commensals) • Indwelling catheters (freshly placed, urine aspirated by needle inserted into catheter) (Foley catheter tips not acceptable) • Straight catheter specimens • Suprapubic aspirates (infants or children, recovery of anaerobes) • Cystoscopic collection of urine
Specimen collection • Male: • If not circumcised, draw back the foreskin. • Begin to urinate, but pass the first portion into the toilet. • Collect the mid-portion of urine into the container, and pass the excess into the toilet. • Female: • Squat over the toilet and separate the labia with one hand. • Void the first portion of urine into the toilet. • Collect the mid-portion of urine into the container and pass the excess into the toilet.
Collection of urine specimens • Urine collected in sterile specimen container must be processed within hours, or refrigerated and processed within 24 hours • Urine collected in sterile specimen container with borate preservative should be processed within 24 hours (no refrigeration required)
Catheterized urine • Cleanse periurethral area with soap and water • Insert catheter into bladder • Discard initial urine • Collect specimen in sterile cup • Chronic indwelling Foley catheter • Clamp tubing below junction (or port) • Disinfect with alcohol • Insert needle (on syringe) through port or catheter wall and aspirate. • DO NOT recontamination
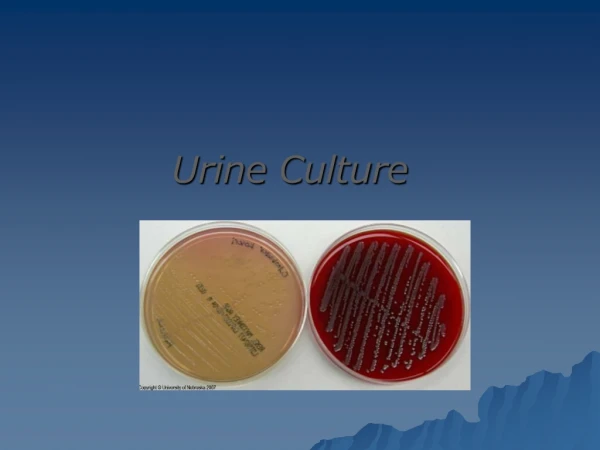
Inoculation of urine • Inoculation of urine for quantitative culture (colony forming units→ CFU’s) performed with a calibrated 0.001 mL(1µL) and 0.01 mL (10µL) plastic or wire loop • Nutrient agar or sheep blood agar utilized for quantitative urine culture • With 0.001 ml loop, 1 colony on SBA equivalent to 1,000 CFU’s per mL of urine • With 0.01 ml loop, 1 colony on SBA equivalent to 100 CFU’s per mL of urine • MacConkey agar utilized as selective differential agar for gram-negative bacteria
Interpretation: Clean Voided Specimen • Normal: <10,000 organisms per ml. • Organisms >10,000 per ml needs repeat urine culture? • Urinary Tract Infection • Boys • Organisms >10,000 per ml suggests UTI likely • Girls • Organisms >100,000 per ml suggests UTI • Three specimens: 95% probability of UTI • Two specimens: 90% probability of UTI • One specimen: 80% probability of UTI
Post specimen processing • Interfering factors: • Patient on antibiotic therapy. • Improper sample collection. • Result reporting: • Report wet mount as an initial report. • Report the isolated pathogen and its sensitivity pattern as a final report. • Turn around time: • Wet mount results should be available 1 hour after specimen receipt. • culture will be reported out 1-2 days after the receipt of the specimen. • Isolation of a possible pathogen can be expected after 2-3 days Negative