Download
1 / 36
360 likes | 506 Vues
WHO OWNS THE BONES?. “Patchwork Quilt” of Women’s Health Who screens? Who treats? Who teaches/ to whom? Whose job it it? Rheumatology Endocrinology Primary Care Gynecology Gerontology Orthopedics Organizations NOF NAMS ISCD. Overview.

E N D
WHO OWNS THE BONES? “Patchwork Quilt” of Women’s Health Who screens? Who treats? Who teaches/ to whom? Whose job it it? Rheumatology Endocrinology Primary Care Gynecology Gerontology Orthopedics Organizations NOF NAMS ISCD
Overview Prevention and Treatment of Osteoporosis • Demographics • Screening • Prevention/Lifestyle • Risk Factors • Pharmaceuticals • Nutriceuticals
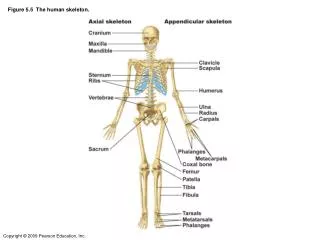
Definition Osteoporosis is a skeletal disorder characterized by compromised bone strength predisposing to an increased fracture risk. BONE DENSITY=BONE DENSITY (70%) + BONE STRENGTH (30%) BONE DENSITY: grams of mineral per area BONE QUALITY: architecture, turnover, damage accumulation, and mineralization NIH Consensus Development Conference on Osteoporosis, 2000
Demographics • 10 Million People have Osteoporosis • 34 Million People have Osteopenia • 1:2 Women will have an osteoporotic fracture in their lifetime • 1.5 Million Fractures Annually • 20% die within one year • $18B Annually www.nof.org
Screening • DEXA is most cost-effective screen today • All women at least 65 yo • Perimenopausal, if risk factors • Any adult > 50 yo with a fracture • Adults with a condition or on a medication associated with bone loss • Patients considering or currently on a medication for osteoporosis • Postmenopausal women considering discontinuation of HRT NOF Clinicians Guide to Prevention and Treatment of Osteoporosis
Densitometry • How often? • Not more than every 2 years • Which bones? • Spine, Hip, Femoral Neck • When to treat? • Osteoporosis • Osteopenia with another risk factor • Lifestyle • Exercise, Calcium, Vitamin D, Smoking, Alcohol • Risk Factors • Age, activity, diet, meds (steroids>3 months), stability, previous fracture, BMI<21,hip fx in a parent, current smoking
Bone Densitometry Values T Score: Standard Deviation comparison of a patient’s bone density to a normal 25 yo. We now have comparison tables by sex and ethnic group. • Normal • T score >-1.0 • Osteoporosis • T score < -2.5 • “Osteopenia” • T score -1.0 to -2.5
FRAX SCOREWHO Fracture Risk Assessment Tool • Uses calculations based on patient data to determine a 10-year risk of hip and major osteoporosis-related fracture • http://www.shef.ac.uk/FRAX/index.htm
NAMS Recommendations Use lowest T-score to define diagnosis Prevention and nutritional measures first Drug Treatment: Any Vertebral Fracture All T-scores < -2.5 Anyone on steroids >3 months T-scores of -2 to -2.5 if one risk factor BMI<21 Fragility Fracture History Hip Fracture History in a Parent
Medical Workup • 25-OH Vitamin D Levels • FSH • TSH • Parathyroid Hormone • Creatinine Clearance • Alkaline Phosphatase • Liver Enzymes • Celiac Antibodies • Protein Electrophoresis • 24-hr. Urine • Calcium, Creatine, Sodium, Free Cortisol
Risk Factors used in FRAX • Geographic Region • Race • Sex • Height/Weight • Previous Fragility Fracture • Family History of Osteoporosis • Current Smoking • Steroid Use (5 mg/da for over 3 months) • Rheumatoid Arthritis • Secondary Osteoporosis • Alcohol (3 or more units daily) • BMD (T score at femoral neck)
So Whom Do We Treat? • Patients with previous hip or vertebral fracture • T score of -2.5 or less at femoral neck, total hip, or spine • T score of -1.0 to -2.5 (Osteopenia) AND: • Other prior fracture • Secondary cause associated with high fracture risk • FRAX risk of 3% or more at hip • FRAX risk of 20% or more for major osteoporosis related fracture at any site
Trends in Treatment Recommendations 2003 2008 Patients with previous hip or vertebral fracture T-score of -2.5 at femoral neck, total hip, or spine T-score of -1 to -2.5 at femoral neck, total hip, or spine AND: Other fracture Other risk factors FRAX of 3% or more at hip FRAX of 20% for other site • Patients with previous hip or vertebral fracture • T-score of -2 at hip • T-score of -1.5 to -2 at hip PLUS additional risk factor.
Treatment Options • Nutrition and Supplements • Exercise • Fall Prevention • Alcohol and Nicotine Avoidance • Pharmaceuticals • Bisphosphanates • SERMs • PTH • HRT • Calcitonin
Bisphosphanates Generic Brand Name Fosamax Actonel Boniva Reclast Aredia Didronel Skelid • Alendronate • Risendronate • Ibandronate • Zoledronic Acid • Pamidronate • Etidronate • Tiludronate
Bisphosphanates • All are indicated for prevention and/or treatment of postmenopausal osteoporosis • Bind permanently to bone to decrease osteoclastic activity and increase bone mass • Concerns about bone quality (“frozen” bone) • Implications for fertility – contraindicated in women planning pregnancy
Bisphosphanates • Similar efficacy • Adverse effects: Esophageal erosion, hypocalcemia, bone pain • Contraindications: esophageal dysmotility, significant renal dysfunction, hypocalcemia • Osteonecrosis of Jaw (ONJ): <1 case/100,000 years of exposure. Usually with high IV doses for cancer Rx. Khann. J.Rheumatol. 2009;Mar;36(3):478-90.
Estrogen Agonist/Antagonist(Formerly called SERMS) Raloxifene (Evista) • Bind to ER, activating some/ blocking others • Decrease vertebral fractures, but no significant effect on hip fractures • One 60 mg tab daily • Adverse Effects: hot flashes, VTE, leg cramps Ettinger et al. JAMA 1999;282:637-645.
Pharmacologic Treatment Options • Anabolics • Teriparatide (Forteo) • Antiresorptives • Calcitonin • Estrogens • SERMS (Raloxifene/Evista) • Bisphosphanates • Alendronate • Risendronate • Ibandronate • Zoledronic Acid
Recombinant Parathyroid Hormone (r-PTH:Teriparatide (Forteo) • Stimulates new bone formation • New fractures are significantly decreased • Vertebral decreased by 65% • Non vertebral decreased by 55% • Concern about malignancies in mice • Dosage • 20 mcg SQ daily for 2 years • Cost - $20. per day Neer, RM, et al. NEJM 2001;344:1434-41
Calcitonin (Miacalcin, Fortical) • Naturally occuring hormone which antagonizes the effects of PTH • Reduces osteoclastic bone resorption • 200 IU intranasal spray achieves 33% reduction in vertebral fractures in postmenopausal women with prior vertebral fractures (PROOF study) Chestnut et al. Am J. Med. 2000;109:267-276.
Compliance FACT After being prescribed a pharmaceutical for osteoporosis or osteopenia, less than 50% of patients have continued therapy at 6 mo • Cost issues • Side effect issues • “Silent Disease” issues How can we affect this statistic???
Lifestyle Issues • Exercise • Calcium • Vitamin D • Medications
Poor Consumption of Vitamin DNHANES III DATA National Health and Nutrition Evaluation Survey J.Amer Diet Assn. 2004:104:980-983
Bone Health Calcium: • 35 RCTs document that calcium prevents or reduces bone loss in adults • Dose • Premenopausal (or on HRT): 1000 mg daily • Postmenopausal: 1500 mg daily Vitamin D: • Oral Vitamin D between 700-800 IU/d significantly reduces the risk of fractures • 400 IU/d is not sufficient for prevention
Working Smarter, not Harder Shared Medical Appointments (SMA) • Basics • Number served • Confidentiality statement • Charges (99214) • 25-40’. 50% Counseling • Dexa SMA • Data reviewed and distributed • Diagnoses established • Lifestyle measures • Therapies discussed
FINISH Thank you
Prescription Nutritionals 3 Primary Concerns for Women’s Health: • Bone Health • Cardiovascular Health • Mental Well-Being Primary Nutrients with Supporting Evidence: • Calcium • Vitamin D • Omega-3 Fatty Acids • Folic Acid • Vitamin B 6
Cardiovascular Health Omega-3 Fatty Acids: • Eskimo observational studies • Nurses Health Study • Physician’s Health Study • RR 0.77 decreased mortality • 850 mg can be expected to save 20 lives per 1000 patients with CHD over 3.5 yrs. Folic Acid • Lowers homocysteine • Improves endothelial function B Vitamins • Nurses Health Study • RR 0.55 of MI in groups with highest levels of Folate and B 6 • SHEEP Study • RR 0.66 of MI in women taking B vitamin supplements Calcium • Significantly increases HDL:LDL Ratio • Suggests 30% reduction in CV events
Mental Well-Being Omega-3 Fatty Acids • Reverses inflammation from Omega-6 and dysmenorrhea • Significant reduction in menstrual symptoms in adolescents Calcium • 48% fewer PMS symptoms than placebo group • Osteoporosis risk much greater in women with history of PMS Folic Acid • Low folate has been linked to depression • Depressed patients have increased homocysteine levels
Prescribing Nutriceuticals Write out above recommendations and send the patient to a pharmacy, healthfood store, Nutritionist, or Sams Club, Or . . . . Prescribe Nutriceuticals ENCORA METAGENICS
Ideal Dosing of Nutritional Supplements for Women Calcium • 1200 mg for women >51 (IOM) • Doses >500 mg should be divided • Better utilized if larger dose is at HS Vitamin D • 400 IU (IOM) wrong • New evidence suggests 700-800 IU • Needed to absorb calcium and prevent hyperparathyroidism Omega-3 Fatty Acids • 500/d in those at risk for CHD • 1000 mg/d if documented CHD (AHA) Folic Acid • 400 mcg/d (IOM) • 0.8-5 mg being studied for CV benefit • Larger dose in AM (prime time for MI)