NECROTIZING ENTEROCOLITIS
NECROTIZING ENTEROCOLITIS. Janice Nicklay Catalan M.D. OBJECTIVES. Ability to diagnose and treat the signs and symptoms of NEC Ability to evaluate radiographs for the classic findings of NEC List several long-term complications associated with NEC. NECROTIZING ENTEROCOLITIS.

NECROTIZING ENTEROCOLITIS
E N D
Presentation Transcript
NECROTIZING ENTEROCOLITIS Janice Nicklay Catalan M.D.
OBJECTIVES • Ability to diagnose and treat the signs and symptoms of NEC • Ability to evaluate radiographs for the classic findings of NEC • List several long-term complications associated with NEC
NECROTIZING ENTEROCOLITIS • Epidemiology: • most commonly occurring gastrointestinal emergency in preterm infants • leading cause of emergency surgery in neonates • overall incidence: 1-5% in most NICU’s • most common in VLBW preterm infants • 10% of all cases occur in term infants
NECROTIZING ENTEROCOLITIS • Epidemiology: • 10x more likely to occur in infants who have been fed • males = females • blacks > whites • mortality rate: 25-30% • 50% of survivors experience long-term sequelae
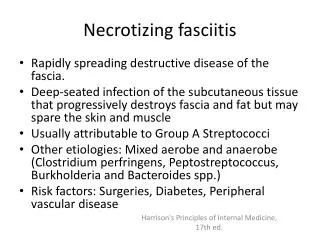
NECROTIZING ENTEROCOLITIS • Pathology: • most commonly involved areas: terminal ileum and proximal colon • GROSS: • bowel appears irregularly dilated with hemorrhagic or ischemic areas of frank necrosis • focal or diffuse • MICROSCOPIC: • mucosal edema, hemorrhage and ulceration
NECROTIZING ENTEROCOLITIS • MICROSCOPIC: • minimal inflammation during the acute phase • increases during revascularization • granulation tissue and fibrosis develop • stricture formation • microthrombi in mesenteric arterioles and venules
NECROTIZING ENTEROCOLITIS • Pathophysiology: UNKNOWN CAUSE…….
CIRCULATORY INSTABILITY Hypoxic-ischemic event Polycythemia PRIMARY INFECTIOUS AGENTS Bacteria, Bacterial toxin, Virus, Fungus MUCOSAL INJURY INFLAMMATORY MEDIATORS Inflammatory cells (macrophage) Platelet activating factor (PAF) Tumor necrosis factor (TNF) Leukotriene C4, Interleukin 1; 6 ENTERAL FEEDINGS Hypertonic formula or medication Malabsorption, gaseous distention H2 gas production, Endotoxin production
RISK FACTORS • Prematurity: • primary risk factor • 90% of cases are premature infants • immature gastrointestinal system • mucosal barrier • poor motility • immature immune response • impaired circulatory dynamics
RISK FACTORS • Infectious Agents: • usually occurs in clustered epidemics • normal intestinal flora • E. coli • Klebsiella spp. • Pseudomonas spp. • Clostridium difficile • Staph. Epi • Viruses
RISK FACTORS • Inflammatory Mediators: • involved in the development of intestinal injury and systemic side effects • neutropenia, thrombocytopenia, acidosis, hypotension • primary factors • Tumor necrosis factor (TNF) • Platelet activating factor (PAF) • LTC4 • Interleukin 1& 6
RISK FACTORS • Circulatory Instability: • Hypoxic-ischemic injury • poor blood flow to the mesenteric vessels • local rebound hyperemia with re-perfusion • production of O2 radicals • Polycythemia • increased viscosity causing decreased blood flow • exchange transfusion
RISK FACTORS • Enteral Feedings: • > 90% of infants with NEC have been fed • provides a source for H2 production • hyperosmolar formula/medications • aggressive feedings • too much volume • rate of increase • >20cc/kg/day
RISK FACTORS • Enteral Feedings: • immature mucosal function • malabsorption • breast milk may have a protective effect • IGA • macrophages, lymphocytes • complement components • lysozyme, lactoferrin • acetylhydrolase
Gestational age: < 30 wks 31-33 wks > 34 wks Full term Age at diagnosis: 20 days 11 days 5.5 days 3 days CLINICAL PRESENTATION • Time of onset is inversely related to gestational age/birthweight
Gastrointestinal: Feeding intolerance Abdominal distention Abdominal tenderness Emesis Occult/gross blood in stool Abdominal mass Erythema of abdominal wall Systemic Lethargy Apnea/respiratory distress Temperature instability Hypotension Acidosis Glucose instability DIC Positive blood cultures CLINICAL PRESENTATION
Sudden Onset: Full term or preterm infants Acute catastrophic deterioration Respiratory decompensation Shock/acidosis Marked abdominal distension Positive blood culture Insidious Onset: Usually preterm Evolves during 1-2 days Feeding intolerance Change in stool pattern Intermittent abdominal distention Occult blood in stools CLINICAL PRESENTATION
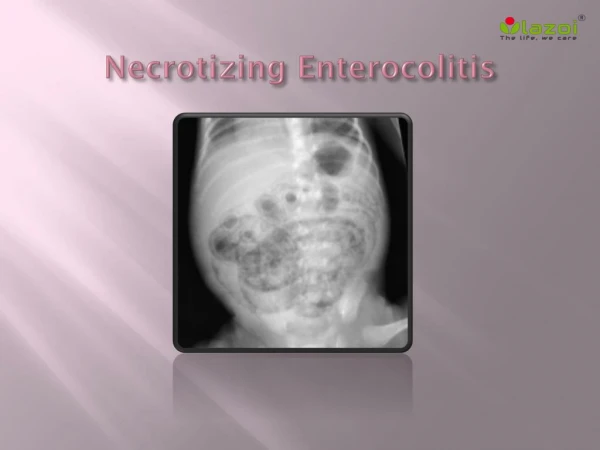
RADIOLOGICAL FINDINGS • Pneumatosis Intestinalis • hydrogen gas within the bowel wall • product of bacterial metabolism • a. linear streaking pattern • more diagnostic • b. bubbly pattern • appears like retained meconium • less specific
RADIOLOGICAL FINDINGS • Portal Venous Gas • extension of pneumatosis intestinalis into the portal venous circulation • linear branching lucencies overlying the liver and extending to the periphery • associated with severe disease and high mortality
RADIOLOGICAL FINDINGS • Pneumoperitoneum • free air in the peritoneal cavity secondary to perforation • falciform ligament may be outlined • “football” sign • surgical emergency
LABORATORY FINDINGS • CBC • neutropenia/elevated WBC • thrombocytopenia • Acidosis • metabolic • Hyperkalemia • increased secondary to release from necrotic tissue
LABORATORY FINDINGS • DIC • Positive cultures • blood • CSF • urine • stool
TREATMENT • Stop enteral feeds • re-start or increase IVF • Nasogastric decompression • low intermittent suction • Antibiotics • Amp/Gent; Vanc/Cefotaxime • Clindamycin • suspected or proven perforation
TREATMENT • Surgical Consult • suspected or proven NEC • indications for surgery: • portal venous gas; pneumoperitoneum • clinical deterioration • despite medical management • positive paracentesis • fixed intestinal loop on serial x-rays • erythema of abdominal wall
TREATMENT • Labs: q6-8hrs • CBC, electrolytes, DIC panel, blood gases • X-rays: q6-8hrs • AP, left lateral decubitus or cross-table lateral • Supportive Therapy • fluids, blood products, pressors, mechanical ventilation
PROGNOSIS • Depends on the severity of the illness • Associated with late complications • strictures • short-gut syndrome • malabsorption • fistulas • abscess * MOST COMMON