Download
1 / 42
420 likes | 447 Vues
Learn about the diagnosis, treatment, and epidemiology of digestive tract diseases in HIV-infected children, including oral candidiasis and diarrhea. Explore the common causative pathogens and clinical manifestations of diarrhea, and develop a treatment plan for HIV-infected children.

E N D
Digestive Tract Diseases in HIV-infected Children HAIVN Harvard Medical School AIDS Initiative in Vietnam
Learning Objectives By the end of this session, participants should be able to: • Diagnosis and treatment of oral candidiasis • Describe the most common causative pathogens of diarrhea in HIV-infected children • Describe clinical manifestations and diagnosis of diarrhea • Develop a treatment plan for diarrhea in an HIV-infected child
Oral Candidiasis • Common seen in severe stage of immunodeficiency • Usually persistent and refractory • Form: • multiple white • easily removable patches • pseudomembranous plaques • Place • Tongue • Gums • Buccal and pharyngeal mucosa • Esophagus
Oral Candidiasis • Diagnosis: • Clinically • Eosophagoscopy • Microscopic exam • Culture
Esophageal Candidiasis • Dysphagia/ painful swallowing • Post chest pain • Nausea, vomiting • Fever Spsuedomembrane plaques on eosopaheal wall
Treatment • Topical: • Clotrimazole (Dartarin cream) • Ketoconazole • Nystatin • Systemic: Source: National guidelines 3003, 2009
Definition Diarrhea is defined as having loose or watery stool at least 3 times per day, or more frequently than normal WHO 2009. Diarrhea: why children are still dying and what can be done
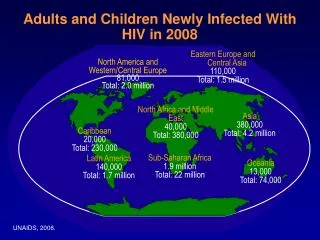
Epidemiology • Diarrhea is the second leading cause of death among children less than 5 years old • Diarrhea occurs more frequently in HIV-infected children than in HIV-negative children, with more severe and persistent episodes WHO 2009. Diarrhea: why children are still dying and what can be done
Etiology (1) • The most common diarrheal pathogens in children include: • Rotavirus • Bacterial agents • In addition, HIV-infected children are susceptible to other less common pathogens: • Protozoans • Parasites • Mycobacteria WHO 2009. Diarrhea: why children are still dying and what can be done
Etiology (2) HIV-associated Pathogens: occurs in severely immunosuppressed children • Cryptosporidium infection • MAC infection • Abdominal TB lymph node infection • Cytomegalovirus (CMV) • CMV-associated Colitis
Etiology (3) • Other causes are non-infectious etiologies: • HIV-associated malabsorption • Lactose intolerance • Medication side effects: • Didanosine (ddI), buffer form • Protease inhibitors (PI): • Lopinavir/ritonavir • Ritonavir
Pathogenesis (1) • Factors that contribute to susceptibility to diarrhea in HIV-infected children: • young age • malnutrition • undernourishment • immunocompromised status
Pathogenesis (2) • Micronutrient deficiency increases risk of mortality several fold • Diarrhea is transmitted through: • Fecal-oral route • Contaminated food and water • Person-to-person
Diagnosis: Overview • Recognize diarrhea is important as delayed diagnosis and treatment would result in patient mortality • Focus on history can classify the diarrhea, its severity, and its possible causes • Physical exams are also important to assess illness severity
Diagnosis: History (1) • Onset: acute, subacute • Duration: how long • Number of bowel movements a day • Stool characteristics • Profuse • Watery • Semi-form • Mucous • Bloody
Diagnosis: History (2) • Associated symptoms: • Fever, vomiting, abdominal pain. • Other household members with diarrhea • Other history: • Medications (ARVs, other drugs) • Food/water intake • Other OI that may cause diarrhea
Symptoms/Signs Associated with Dehydration • Mental status • Thirst • Heart rate • Quality of pulses • Breathing • Eyes • Tears • Mouth and tongue • Skinfold • Capillary refill • Extremities • Urine output
CMV-associated Colitis • Sigmoidoscopy: disseminated unspecific rash, sub-mucous bleeding and ulcer • Histology: inclusion body in intracytoplasma
Overview • In general, most diarrheal illness does not require laboratory testing • However, in cases of severe or persistent diarrhea, the following tests may be useful: • CBC • Electrolytes • Renal functions • Blood culture
Stool Study • Stool microscopic exam: WBC, RBC, O&P • Stain: AFB, Modified AFB • Antigen detection: • Rotavirus antigen • C. difficile toxin • Stool culture: • Bacteria • Mycobacterium species Chronic diarrhea not responsive to usual therapy: Sigmoidoscopy, Colonoscopy
Treatment Fluid replacement and feeding!!!
Treatment at Home • Give the child more fluid than usual • Fluid replacement: low osmolality oral rehydration solution (ORS) or home made solution • <2 years old: 50-100 ml after each watery stool • Older child: 100-200 ml • Zinc supplement: • younger than 6 months: 10mg daily; • 6 months and older: 20 mg daily for 2 weeks • Continue feeding: • Breast feeding: continue and more frequently • Formula feeding: every 3 hours • Soft food: continue with addition of milk
Treatment at Home • When to return • Begins passing frequent, watery stools • Has repeated vomiting • Becomes very thirsty • Is eating or drinking poorly • Develops a fever • Has blood in the stool • Does not get better in 3 days
Inpatient Treatment (1) For mild and moderate dehydrated cases, admission to the hospital is necessary • Oral rehydration: 75 ml/kg for 4 hours • Monitor if the ORS given appropriately • Assess during and after 4 hours, if any sign of severe dehydration detected, IV replacement is needed • Zinc supplement: after first 4 hours as treatment at home • Feeding: • encourage breast feeding whenever possible • Other: as treatment at home
Inpatient Treatment (2) For severe dehydrated • IV rehydration with lactate ringer/normal saline solution • If IV not available: nasogastric tube can be used to give ORS • Oral rehydration in addition • Correction of acidosis, electrolyte repletion • Zinc supplement and feeding when possible
ShigellosisSalmonellosis (bloody stool) • Ciprofloxacin: 15 mg/kg/day BID x 5 days • Norfloxacin: 15 mg/kg/day BID x 5 days • Cephalosporin 3th gen • Ceftriaxone: 50 mg/kg IV x 5 days • For H.histolytica: • Metronidazole: 50 mg/kg/day TID x 5 days
HIV-associated Pathogens ARV is the common treatment
A 2-year-old child comes to your OPC for follow-up His mother mentions to you that he has been having diarrhea for the last 2 days He has 5-6 stools per day. The stool is watery, non-bloody, without mucous The mother thinks he also runs a fever because his forehead feels hot to the touch His most recent CD4: 25%, 500cps/ml He’s not yet on ARV Case Study
Key Points • Diarrhea is common in HIV-infected children and needs aggressive treatment • Most common pathogens are viruses, bacteria and local circulating agents • OIs causing diarrhea include TB, MAC, cryptosporidia and CMV
Thank you! Questions?