Download
1 / 27
280 likes | 449 Vues
Leadership Accountability Demonstration Project. Horizontal Learning Call/Intensive Group October 15, 2014. Overview. Presentation by Cohort 1 Team Jennings American Legion Brief Cohort 2 Team Updates Our Lady of the Lake Holy Redeemer Discussion and next steps.

E N D
Leadership Accountability Demonstration Project Horizontal Learning Call/Intensive Group October 15, 2014
Overview • Presentation by Cohort 1 Team • Jennings American Legion • Brief Cohort 2 Team Updates • Our Lady of the Lake • Holy Redeemer • Discussion and next steps Armstrong Institute for Patient Safety and Quality
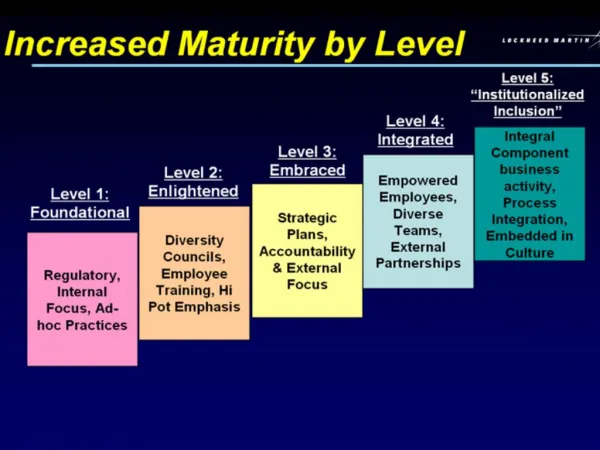
Overview: Model of Accountability Armstrong Institute for Patient Safety and Quality
Leadership Accountability Project VTE prophylaxis HEN Jennings American Legion Hospital
Aligning Goals • Goal = 100% VTE prophylaxis • Goal applied to each unit and each physician • Progress toward goal discussed at all levels • Weekly progress reports for the units • Monthly progress reports for the physicians
Physician Scores Dr XXXX Ordered on admit9/15 = 60% Received after screen 2/4 = 50% ( only patients who screened at risk are included) 9 of 15 patients had VTE prophylaxis addressed upon admission. 4 were screened at risk, 2 did not receive prophylaxis within 24 hrs of admit. Patient X – no medication and no contraindication given Patient Y – no medication and no contraindication given
Accountability • Daily calls to units • Needed to hardwire the accountability • Charge Nurse Check List was developed
Brief Team Updates Armstrong Institute for Patient Safety and Quality
Our Lady of the LakeWhat have you been working on to date? • Completed the “Aligning the Goals” tool with each stakeholder group. Within each group we decided to focus on 2-3 components of CLABSI prevention-some were group specific and some more organizational specific. • We have a CLABSI workgroup that meets weekly on one of the 3 selected pilot units (MICU, SICU, and STU). We meet at the nursing station and encourage frontline staff involvement in these workgroup meetings. Overall, our focus will be to ensure that all clinicians know the CLABSI data of their specific area and of the organization. • To hardwire our current central line checklist, and ensure bedside clinicians are empowered to speak up when there is a break in compliance. Med Staff has agreed to support the nursing team as we hold inserting practitioners accountable to our standard inserting procedures. Armstrong Institute for Patient Safety and Quality
Our Lady of the LakeWhat’s next for your team? • We will continue to meet weekly tracking data and trends utilizing a weekly Infection List that provides “real time” data regarding infections. The list includes patient specifics and gives the units involved. The list is sent to unit managers via email and allows for the manager to complete a Defect Analysis on the infection(s). • The findings of the defect analyses are compiled and attached to the Weekly infection list spreadsheet/email. Trends and opportunities are monitored through this process. Our focus will be on ensuring the CL checklist is completed with every insertion and that the staff feels empowered to speak up. • We are planning to have our Virtual ICU nurse complete the checklist and monitor compliance with CL insertion standards. • We also send a personal letter to any physician that inserted a CL that has been determined to have caused a CLABSI. Armstrong Institute for Patient Safety and Quality
Our Lady of the LakeWhat are the key lessons you’ve learned so far you would like to share, or what are the key questions you would like to ask the group? • Data has shown that compliance with the CL Checklist has proven to be most impactful. • Physician Champions are a key component to ensuring compliance and accountability throughout the organization. • Having Managers and staff complete a defect analysis on every CLABSI event seems to be raising awareness. • Making Data (Unit performance) easily accessible raises awareness and demonstrates the importance of meeting the goal of “0” CLABSI events. Armstrong Institute for Patient Safety and Quality
Holy Redeemer HospitalWhat have you been working on to date? • Communication methodology for all constituents (boards/ huddles/ letters) • Education of nursing staff on new infection control bundle for hips- completed • Letters to staff for both projects: falls- completed, SSI- in process Armstrong Institute for Patient Safety and Quality
Holy Redeemer HospitalWhat’s next for your team? • Implement new components of SSI bundle • Hardwiring walking program for consistency for falls in SBHU • Development of action plan based on survey results Armstrong Institute for Patient Safety and Quality
Holy Redeemer HospitalWhat are the key lessons you’ve learned so far you would like to share, or what are the key questions you would like to ask the group? Key lessons: Verbal sharing of data is beneficial if the receiver acknowledges and acts on information shared. Moving to multiple modalities to communicate with staff. Question: Staff and physician engagement, how to conquer this frontier? Armstrong Institute for Patient Safety and Quality
Holy Redeemer HospitalTotal Hip and Bipolar Hip Infection Rates FY 2013 1.0 FY 2014 7.8
Holy Redeemer HospitalC-section Infection Rates FY 2013 0.3 FY 2014 0.7
Holy Redeemer HospitalFY 2015 Infection Rates Total Hips & Bipolar Hips 0 C-sections 0.4
Holy Redeemer HospitalFalls: Acute Care Armstrong Institute for Patient Safety and Quality
Holy Redeemer HospitalFalls/SBHU SBHU:There were five falls.Rate = 13.5 (Threshold = 8.5) Four of the five falls occurred on evening shift between 16:50-21:00 The falls occurred on Sunday (3), Monday (1) and Friday (1). The average age of patients who fell = 80. Injuries: Laceration w Steri Strips. OUT PATIENTS:There were two outpatient falls: EMG and SDS. Armstrong Institute for Patient Safety and Quality
Holy Redeemer HospitalFalls Alert Calendar Armstrong Institute for Patient Safety and Quality
Dear Team Member: Welcome to Holy Redeemer’s Senior Behavioral Health Unit. As part of our commitment to Safe Care, we are dedicated to reducing. The number of patient falls and injuries on our unit. Reducing falls requires a team effort. As a team member you play an important role in preventing falls. SBHU FALL PREVENTION GUIDE: Fall prevention begins with knowing your patient: ● Please take a few minutes at the start of your shift to acquaint yourself with our patients and their specific risk factors for falls. This information can be found in the nursing assessments. ● Please make sure that you receive a thorough report from the previous shift. ● Communication between our RNs and PCA is vital when it comes to the use of PRN medications, as their use may result in sedation and/or complicate ambulation. It is also important to be familiar with our environment of care. Falls can happen any place on the unit. ● Please take a few minutes to observe the unit and remove anything that could clutter hallways and patient rooms. ● Two areas in which our patients are prone to fall are in the dining room and the bathroom in the patient’s room. ● All beds should be lowered to the setting closest to the floor. One of our most important fall reduction initiatives is our Walking Program. Each patient should be walked with assistance as needed at least two times a day. ● Best times for walking is 10:00 and 13:00 PM. Please document this activity on our Walking Program Log. ● If a patient is unable to walk, chair or stationary exercises can be utilized. (Sittercise) ● Of course assisting patient to walk or exercise at other times, depending on the activity level on the unit can also be helpful in this regard and will be much appreciated by our patients and their families. Some of our patients may be restless and/or have difficult to manage behaviors. Lap buddies, when used with wheelchairs, can be very effective with patients who have periods of restlessness. We will sometimes place a patient on one-one observation if it becomes difficult to manage their behaviors. ● Sometimes a patient on one-to-one status may spend a portion of the shift sleeping. It is important to remain vigilant if this occurs as our patients may wake up suddenly and engage in impulsive behaviors. ● While the patient is awake make an effort to engage or occupy the patient in conversation or encourage other activities. ● Please know that if you are assigned to provide one-to-one care that does not mean that you have sole responsibility for caring for the patient. It is important to ask for assistance if you need help in toileting or other related activities. Thank you for everything you do to prevent falls! Holy RedeemerSample Staff Letter Armstrong Institute for Patient Safety and Quality
discussion Armstrong Institute for Patient Safety and Quality
Next Steps • Continue to work on the previous tools • Try the Informal Learning Tracer Tool • Please send it back before next cohort call • Use your Safety Competencies Across your Organization Tool to complement this! Armstrong Institute for Patient Safety and Quality
What’s next? • Next Cohort Call • November 17th • Business case development for safety Armstrong Institute for Patient Safety and Quality
What’s next (con’t)?... Project close out End as planned Extend into 2014 Additional cohort call in January Additional coaching calls Re-administer HSOPS and PSOA (Jan / Feb) Individual survey debriefing calls in March • December will be the final call • Due to late start date and compressed schedule we would not re-administer the surveys Armstrong Institute for Patient Safety and Quality