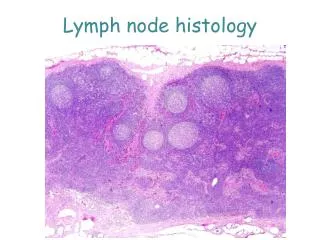
Lymph node pathology
Lymph node pathology. Hodgkin lymphoma or Hodgkin Disease From cases of the Pathology Department - U.M.F. “Gr. T. Popa” Iasi. Fig.23.1.

Lymph node pathology
E N D
Presentation Transcript
Hodgkin lymphoma or Hodgkin DiseaseFrom cases of the Pathology Department - U.M.F. “Gr. T. Popa” Iasi Fig.23.1 • Fig. 23.1. SR cell: Large binucleate cell, (mirror image) with abundant amphofilic cytoplasm and large eosinophilic nucleoli surrounded by a clear halo (appearance of "owl-eye").
Classical Sternberg Reed (SR) cell and variants of SR cells Fig. 23.2 From: Stevens A. J Lowe J. Pathology. Mosby 1995
Hodgkin DiseaseFrom: Stevens A. J Lowe J. Pathology. Mosby 1995 Fig.23.3 Fig. 23.3. Involved lymph nodes are increased in volume, with LN structure completely replaced by gray - white tumoral tissue; LNs retain their individuality, but become adherent between them and deep plans.
Fig. 23.4 Fig. 23.4. Large spleen presents multiple tumoral nodules, of various sizes, white-gray in color separated by red-brown normal splenic parenchyma (appearance of rustic sausage or salami).
Stage I (A sau B)/ IE Single node involvement Stage II / Stage II E Two or more nodes on same side of diaphragm Stage III Lymph nodes on both sides of the diaphragm Spleen involvement Stage IV Diffuse extranodal involvement A = no additional symptoms B = weight loss, night sweats, fever E- extra LN involvement LH – Ann Arbor stagingFrom: Stevens A. J Lowe J. Pathology. Mosby 1995- fig 5From cases of the Pathology Department - U.M.F. “Gr. T. Popa” Iasi-fig 6 Fig. 23.5
Fig. 23.6 Fig. 23.6. In Mixtcellularity Hodgkin lymphoma, lymph node architecture is destroyed and replaced with: (a) a proliferation of tumoral cells (classical SR cells, pleomorphic SR cells, and Hodgkin cells), and (b) reactive non-tumoral cells (lymphocytes, plasma cells, eosinophiles, macrophages), neoangiogenesis, and diffuse fibrosis.
Nodularsclerosis Hodgkin DiseaseFrom cases of the Pathology Department - U.M.F. “Gr. T. Popa” Iasi Fig. 23.7
Fig. 23.8 Fig. 23.7-8. In nodularsclerosis Hodgkin lymphoma the lymph node structure is replaced by tumoral nodules surrounded by fibrotic bands. Tumoral nodules contain: (a) tumoral cells (lacunar cells and classical SR cells) and (b) reactive cellular elements (eosinophiles, T lymphocytes, plasma cells, and histiocytes).
Non-Hodgkin LymphomaFrom: Stevens A. J Lowe J. Pathology. Mosby 1995 Fig. 23.9 Fig. 23.9. Non-Hodgkin Lymphoma-deep abdominal lymphoadenopathy: Deep abdominal lymph nodes mass with tendency to fussion.
Fig. 23.10. Non-Hodgkin Lymphoma-deep mediastinal lymphoadenopathy: Mediastinal homogenous, gray tumoral block with irregular margins resulted by fusion of the tumoral lymph nodes which lost their individuality. Fig. 23.10
Small Lymphocytic LymphomaFrom: Stevens A. J Lowe J. Pathology. Mosby 1995 - fig.11From cases of the Pathology Department - U.M.F. “Gr. T. Popa” Iasi-fig.12 Fig. 23.11
Fig. 23.12 Fig. 23.11-12. Lymph node architecture is replaced by tumoral cells resembling with mature lymphocytes. Tumoral cells infiltrate lymph node capsule.
Hepatic chronic myeloid leukemiaFrom cases of the Pathology Department - U.M.F. “Gr. T. Popa” Iasi Fig. 23.13
Fig. 23.14 Fig. 23.13-14. Liver is infiltrated by pleomorphic leukemic cells (few blast cells, numerous myelocyte cells and metamyelocyte cells and numerous mature neutrophils and eosinophiles), predominantly along of sinusoids.
Hepatic chronic lymphocytic leukemiaFrom cases of the Pathology Department - U.M.F. “Gr. T. Popa” Iasi Fig. 23.15
Fig. 23.16 Fig. 23.15-16. Leukemic lymphocytic infiltrate is localized predominantly in the portobilliary space, which is expanded.