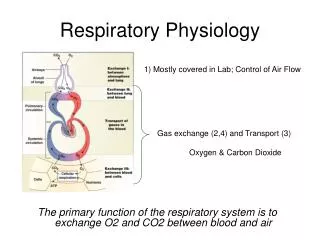
Basic respiratory physiology including oxygen therapy
Basic respiratory physiology including oxygen therapy. Dr Felix Woodhead Consultant Respiratory Physician. Aerobic respiration. Occurs in mitochondria Chemiosmotic synthesis of ATP Final sink for electrons O 2 consumed, CO 2 generated RQ = [CO 2 ]/[O 2 ]

Basic respiratory physiology including oxygen therapy
E N D
Presentation Transcript
Basic respiratory physiology including oxygen therapy Dr Felix Woodhead Consultant Respiratory Physician
Aerobic respiration • Occurs in mitochondria • Chemiosmotic synthesis of ATP • Final sink for electrons • O2 consumed, CO2 generated • RQ = [CO2]/[O2] • C6H12O6 + 6 O2 → 6 CO2 + 6 H2O (RQ=1) • C16H32O2 + 23 O2 → 16 CO2 + 16 H2O (RQ = 16/23 = 0.7)
CO2 • Soluble • Stored as HCO3- (catalysed by CA) • Carboxyhaemoglobin • Linear relationship CaCO2 and pCO2
O2 • Much less soluble in water • Most stored as oxyhaemoglobin • Non-linear relationship (sigmoid) • Flat top → loading still occurs if PAO2 ↓ • Maintains good pressure gradient along alveolus • Steep portion assists off loading in tissues • Shifted to right by temp, acid and pCO2
Acid-base: CO2 • H2CO3 → H+ + HCO3- • K`A = ([H+] x [HCO3-])/[H2CO3] • KA = [H+] x [HCO3-] /[CO2] • log KA = log [H+] + log ([HCO3-])/[CO2]) • - log [H+] = - log KA + log ([HCO3-])/[CO2]) • pH = pKA + log ([HCO3-])/[CO2])
Control of ventilation • Acidity of brain stem • Blood-brain barrier imperm to ions, perm to CO2 • ↑pCO2 → ↓pH • CSF few proteins → pH changes quickly • pCO2 kept very steady • ↑pCO2 implies ventilatory failure • Gradual ↑ HCO3- by kidney to compensate • Low pO2 only relevant in chronic vent insufficiency
Partial pressures • Total pressure = sum of partial pressures of constituent gases • Atmosphere predom N2 (80%) and O2 (20%) • patm = pN2 +pO2 • FiO2 = fraction inspired O2 = 0.20 • 1 atm = 100 kPa • pO2 (at sea level) = 20 kPa
A-a gradient • Idealised lung arterial pO2 same as alveolar • Alveolar pO2 = inhaled pO2 – used up O2 • Used up O2 related to generated CO2 by RQ • pAO2 = pIO2 – (pCO2/R) • A-a gradient = pAO2 - paO2 • Fudge factor for pACO2 + pAH20 ≈ 5 • Greater A-a gradient implies problem with lungs (V/Q mismatch)
V/Q ratio • V/Q = 0 • Shunt • PaO2 → mixed venous pO2 • V/Q = ∞ • No flow • Gases approximate PAO2 but ventilation wasted • V/Q mismatching • always → ↓pO2 (A-a gradient ↑) • pCO2 may be normal as total vent ↑
Partial pressure vs concentration • In a perfect gas pp prop conc • In a liquid, depends on solubility and chemical binding • Pp like voltage determines diffusion • Concentration like thermal energy depends on material
Oxygen carriage • Depends on cardiac output, [Hb] and SaO2 • Once Hb saturated O2 stored dissolved • ↑ FiO2 →↑ pO2 ++ but only ↑ CaO2 a little • Possible to ↑ pO2 without ↑ CaO2 • pO2 affects rate of diffusion and control of breathing • Cannot increase pO2 of individual alveolar units by ↑ ventilation
Respiratory Failure • pO2 < 8 kPa • Type I • Normal/low pCO2 • V/Q mismatch/diffusion limitation • Ventilation able to compensate • Type II • ↑ pCO2 • ↓pH if acute • Ventilatory failure • Needs controlled O2± ventilation
O2 or ventilation • Is there impaired ventilation? • If there is impaired ventilation is it the only problem or is it part of multi-organ failure? • Is invasive ventilation appropriate?
O2 delivery systems • High flow vs low flow systems • Does flow rate exceed minute ventilation? • Low flow rates, FiO2 ↑ with ↓ minute vent • Nasal specs comfortable and cheap, not for acutely unwell • High flow FiO2 independent of vent rate (Venturi) • Non-rebreathing (reservoir bag) • Higher pO2 requires complete seal
Basic respiratory anatomyincluding radiology Dr Felix Woodhead Consultant Respiratory Physician
Lobes • Heart on left • 3 lung lobes on Right • 2 lobes on left • Left main bronchus deviates horizontally to miss heart • RMB straighter (inhaled foreign body) • Lingula (tongue) is analogous to RML, arises LUL • Upper and lower lobes pyramidal • Lower lobes one apical and four basal segs • Oblique (major) fissure bilat (seen on lat), horizontal only on R (PA)
Radiological patterns 1 • Pleural effusions/mass • Dense white with no air bronchograms • Meniscus • Beware the supine effusion • Tumours • Spiculated & single (primary) vs round & multiple (mets) • May present as collapse • Collapse • Volume loss (shift of fissure/hilum) • Obliteration of adjacent silhouette
Alveolar space filling (≡ consolidation) • Fairly dense, with air bronchograms (patent airways) • Neutrophils ± microrganisms (pneumonia/organising pneumonia) • Eosinophils (eosinophilic pneumonia) • Blood (pulm haemmorhage) • Fluid (severe pulm oedema) • Surfactant (alveolar proteinosis) • Tumour (bronchoalveolar carcinoma – BAC)
Interstitial shadowing • Less dense than consolidation, dots and lines on CXR (reticulonodular) • Interstitial fluid (pulm odema) • Trapped lymph (lymphangitis carcinomatosis) • Inflammation/fibrosis • Interstitial lung disease • Diffuse parenchymal lung disease • Fibrosing alveolitis • “pulmonary fibrosis”
An approach to chest radiographs • Normal or abnormal? • If abnormal, how long? • If consolidation ?pneumononia • treat with antibiotics and repeat film 6-8/52 • If interstitial ?pulm oedema • Treat with diuretics and repeat film in a few days • Remember • Not all LRTIs are pneumonia (bronchitis/bronchiectasis) • Pulm oedema also seen with fluid resus and renal pts • Long-standing shadowing ?diffuse parenchymal lung disease
CT radiology terminologyFleischner Society: Glossary of Terms for Thoracic Imaging Radiology 2008 246 697-722
CXRs vs CTs • CXR • Cheap • Quick • Good screen • Serial change • Low radiation dose • CT • Better spatial resolution • Staging • Patterns of disease • ?too sensitive