Download
1 / 20
330 likes | 4.83k Vues
Pathomechanics of Knee Joint (part II). 4 th Lecture Biome II Dr . Manal Radwan Salim Lecturer of Physical Therapy Tuesday 22-10-2013 Saturday 26-10-2013 . 3- Mensicial Tears.

E N D
Pathomechanics of Knee Joint (part II) 4th Lecture Biome II Dr . ManalRadwanSalim Lecturer of Physical Therapy Tuesday 22-10-2013 Saturday 26-10-2013
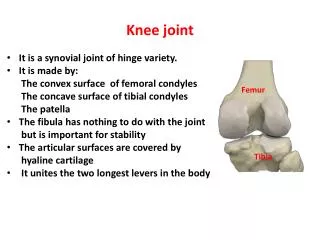
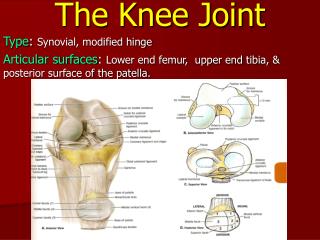
3- Mensicial Tears Medial and lateral meniscus are fibrocartilagenous discs that deepen the shallow articular surface of tibia by acting as seats or cushions to femoral condyles. Medial meniscus is C shaped while lateral meniscus is 0 shaped. Functions of menisci: 1-Reduce the huge compressive stress at the tibio-femoral joint that may reach 2-3 times body weight during routine knee activity by 230% through trippling the area of joint contact. 2- Stabilizing the joint during motion. 3-Lubricating the articular cartilage. 4-Reducing friction.
Attachments of Menisci: Attachments of menisci; although help to stabilize menisci in place, but also loose enough to allow menisci to pivot freely during movement of knee joint. Position of menisci is controlled by the muscular attachments in active motion so they don’t normally lock knee while moving. *Both menisci are attached to: 1-each other anteriorly, 2--tibial plateau, 3-femoral condyles, 4-joint capsule, 5-quadriceps and 6-semimembrenosus. Additionallymedial meniscus is attached to 7-medial collateral ligament, lateral meniscus is attached to , 8-popliteus muscle. *The medial meniscus is more frequently injured more than lateral meniscus because its attachment to the medial collateral ligaments. As medial meniscus movements are more limited than lateral meniscus movements because.
Common Mechanisms of Injury: -Tears of menisci often occurs by forceful horizontal plane rotations of the femoral condyles over a partially weight bearing flexed knee. -A classic complaint of an individual with a menicscial tear (dislodged or flap meniscus) is that the joint locks when he or she attempts to extend the knee from a position of weight bearing, such as rising from a seated position or climbing stairs.
Treatment of menisceal tear surgery either partial menisectomy or replacement according to extent of injury and degree of degeneration in chronic conditions. Total mensictomy is no longer advised for patients as it lead to increased degeneration process in the knee and accelerated incidence of osteoarthritis because the normal functions of menisci of shock absorption and cushioning effects between two bone ends are eliminated, also the
4- Collateral Ligaments Injury • The medial collateral ligament (MCL):is a flat, board structure that spans the medial side of the joint. • It resist valgus stress (abduction), extension, and extreme axial rotations. • Common mechanism of injury : 1-Valgus force with foot planted, 2- severe hyperextension injury of knee.
b) The lateral (fibular) collateral ligament(LCL): consists of a round strong cord that runs nearly vertical between the lateral epicondyle and head of fibula. It resist varus stress (adduction), extension, and extreme axial rotations. Common mechanism of injury :1-Valgus force with foot planted, 2- severe hyperextension injury of knee.
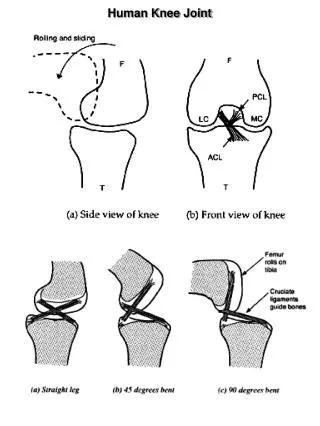
5-Cruciate ligaments injury Attachments of Anterior crusciate ligaments: ACL attaches along anterior condylar area of the tibial plateau, to attach on medial side of the lateral femoral condyle. Most of its fibers are taught when knee approaches full extension .
Functions of (ACL) are: 1- Most fibers resist excessive anterior translation of the tibia or excessive posterior translation of the femur. 2- Limit full knee extension. 3- Resist extremes of varus, valgus and axial rotations.
Mechanisms of injury of ACL: 1- Hyperextension of knee. 2- Large valgus force with foot planted on ground. 3-Either of the above combined with large internal axial rotation torque e.g. the femur forcefully externally rotates over a fixed tibia. Anterior drawer test: Is based on the fact that ACL provide 85% of passive resistance to anterior translation of tibia, so the test is performed with pulling the tibia forward in knee flexed 90 degrees. Anterior translation of 8 mm or 1/3 inch is indicative of a positive ACL injury. It may be masked by hamstring spasm (limiting anterior drawer of tibia).
Relation between muscular contraction and ACL injury: A contraction of quadriceps muscle extends the knee and slides the tibia anteriorly relative to the femur thus increase the tension in most fibers of the ACL. While contraction of the hamstring muscle, in contrast. Causes a posterior translation of the tibia that slackens most fibers of the ACL. Thus in rehabilitation following injuries over strengthening of hamstrings is an essential component
Attatchement of Posterior cruciate ligaments: PCL attaches from the posteriorintercondylar area of tibia to the lateral side of the femoral medial condyle. Become taught in extreme flexion, pulled taught by hamstring contraction and subsequent posterior slide of tibia.
Functions of (PCL) are: 1- Most fibers resist excessive posterior translation of the tibia or excessive anterior translation of the femur. 2- Most fibers taught in full knee flexion. 3- Some fibers are taught at extremes of varus, valgu and axial rotations.
Mechanisms of injury of PCL: 1-Hypeflexion of knee 2- Large valgus or varus force with foot planted . 3- Any of the above, combined with large axial rotation. Testing PCL injury: Posterior drawer test: pushing tibia posteriorly with knee flexed 90 degree Normally the PCL provide 95% degrees of passive resistance to posterior translation of tibia.
Relation between hamstrings and PCL: Contraction of hamstrings muscles flexes the knee and slides the tibia posteriorly relative to the femur thus stressing the posterior cruciateligaments. A contraction of quadriceps muscle extends the knee and slides the tibia anteriorly relative to the femur thus decreases the tension in most fibers of the PCL. Thus in rehabilitation following injuries over strengthening of hamstrings is an essential component Because the cruciate do not spontaneously heal on their on, surgical reconstruction often requires a graft.
6- Patellofemoral disorders The patellofemoral joint is the interface between the articular side of the patella and the intercondylar groove on the femur.
a) Painful Patellofemoral joint Patellofemoral joint pain syndrome is a common conditions, cases may be mild involving only a generalized aching about the anterior knee, or they may be severe and involve recurrent dislocation or sublaxation of the patella from the intercondylar groove. Overtime, some of them develop degenerative changes in the joint surfaces (chondromalacia patellae).
b) Chondromalaciapatellae is charecterized by: 1- excessive cartilage degeneration on the posterior side of the patella. 2-Those with this condition often experience retro-patellar pain and crepitus, especially while squatting or climbing steep stairs or after sitting a prolonged period. 3-The cartilage becomes soft, pitted, and fragmented. Note the irregular surfaces and marked degeneration on the cartilage of the femur and patella
c) Quadriceps Weakness (Extensor lag): Inability to fully extend knee in open kinematic in the last 15 to 20, Although the knee can be fully extended passively; commonly seen in persons with moderate weakness in the quadriceps. Biomechanical causes includes: 1- in moderate weakness as the knee approaches terminal extension, the maximal internal torque potential of the quadriceps is least while the opposing external (flexor) torque is greatest. 2- Swelling or effusion of the knee increases the likelihood of an extensor lag. Swelling increases intra articular pressure, which ca physically impede full knee extension, by reflexively inhibit the neural activation of the quadriceps muscle.
d) Patellectomy It is a condition of removal of the patella. • In this case the patellar tendon lies closer to the center of the tibiofemoral joint than in a normal knee joint so the quadriceps muscle will act with a shorter lever arm, leading to increasing in the force requirements for the muscle. The quadriceps muscle has to develop more tension (about 30%) than is normally required. • So in cases of patellectomy, the patient must be exercised to increase the strength of the quadriceps muscle by about 30% than normal (especially before operation).