Download
1 / 13
250 likes | 3.42k Vues
Pathomechanics of Hip Joint (part II). 6 th Lecture Biome II Dr . Manal Radwan Salim Lecturer of Physical Therapy Tuesday 12-11-2013 . Femoral on pelvic arthrokinematics.

E N D
Pathomechanics of Hip Joint (part II) 6th Lecture Biome II Dr . ManalRadwanSalim Lecturer of Physical Therapy Tuesday 12-11-2013
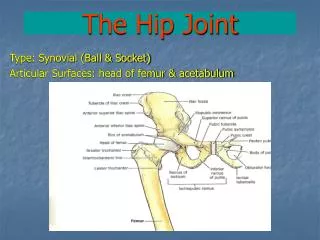
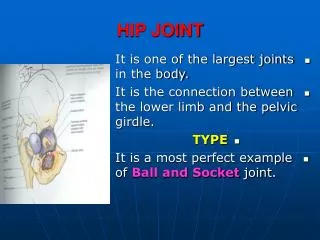
Femoral on pelvic arthrokinematics During hip motion the nearly spherical head remains seated within the boundaries of the acetabulum. The following figure shows a highly mechanically based illustration of the hip opened to enable visualization of the paths of articular motion. *Abduction and adduction occurs across the longitudinal diameter of the joint surfaces(red). *With the hip extended the internal and external rotation occurs across the transverse diameter of the joint surface(grey). *Flexion and extension occurs as spin between the femoral head and the lunate surface of acetabulum.
Femoral on pelvic arthrokinematics/Osteokinematics Flexion/ extension movement of hip in sagital plane: With , knee fully flexed hip flexes to 120 degree, with knee fully extended it flexes with maximum 80 degree due to passive tension within the stretched hamstering and gracillis muscles. * It normally extend to maximum of 20 degree
Abduction/ Adduction movement of hip frontal plane: The hip abducts to 40 degree. * It normally adduct beyond neutral position to maximum of 20 degree
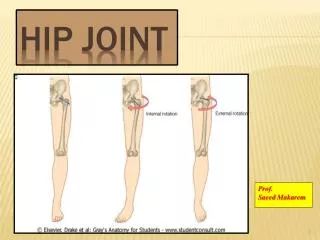
c) internal/external rotation movement of hip in tansverse plane hip internally rotate 35 degree from neutral position. Hip externally rotate about 45 degrees.
Pelvic on femoral osteokinematics:Lumbopelvicrythm The lower caudal end of the axial skeleton is firmly attached to the pelvis by the sacroiliac joint. As a consequence, rotation of the pelvis over the femoral head typically changes the configuration of lumbar spine. A two contrasting types of lumbopelvic rhythm. a)Ipsilaterallumbopelvic rhythm: The pelvis and lumbar spine rotates in same direction, this movements maximizes the angular displacement of the entire trunk relative to lower extreimities, and it is useful for activities such as extending the reaching capacity of upper limb
b) Contralaterallumbopelvic rhythm: The pelvis rotates in one direction while the lumbar spine simultaneously rotates in the opposite direction. The important sequence of this movement is that the supra-lumbar trunk (i.e. part of the body located above the first lumbar vertebrae can remain essentially stationary as the pelvis rotates over femur. This type of rhythm is used during walking and dancing and any other activity in which the position of the supra-lumbar trunk, including the head and eyes need to be held fixed in space, independent of rotation of pelvis.
Pelvic on femoral rotation a) Anterior/posterior pelvic tilt in sagital plane: Hip flexion can occur through a limited arc via an anterior tilt of the pelvis over stationary femoral heads. The direction of anterior or posterior pelvic tilt is based on the direction of rotation of a point on the iliac crest. The associated increased lumbar lordosis offset most of the desired forward motion of the supralumbar trunk In sitting upright with 90 degree hip flexion, the normal adult can achieve about 30 degrees of additional pelvic on femoral flexion before restricted by the fully extended lumbar spine. :
sitting upright with 90 degree hip flexion, the normal adult can achieve about 30 degrees. *The hips can be extended about 10 to 20 degrees from the 90 degrees sitting posture via a posterior tilt of the pelvis. The lumbar spine flexes or flattens as the pelvis is tilted.
Pelvic on femoral rotation in frontal plane Upward and downward rotations in the frontal plane: It is best described in the frontal plane are best described assuming a person is standing on one limb. The weight bearing extremity is referred to as the support hip. Abduction of the support hip occurs by raising or ”hiking” the iliac crest on the side of the non support hip, making 30 degree. *Assuming that the supralumbar trunk remains stationary, the lumbar spine must bend in the direction opposite to the rotating pelvis. A lateral convexity occurs within the lumbar region toward the side of the abducted hip.
Adduction of the support hip occurs by the lowering of iliac crest on the side of the non support hip. This motion causes a slight lateral concavity within lumbar spine region on the side of the adducted hip.
Pelvic on femoral rotation in transverse plane Internal rotation of the support hip occurs as the iliac crest on the side of the non support hip rotates forward in the horizontal plane. During external rotation, in contrast this same iliac crest rotates backwards. If the pelvis is rotating beneath a relatively stationary trunk, the lumbar spine must rotate or twist in the opposite direction as the rotating pelvis.