HIP JOINT
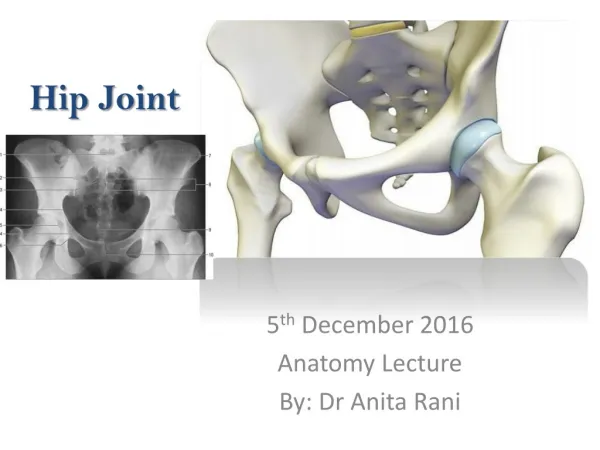
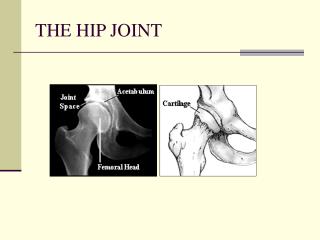
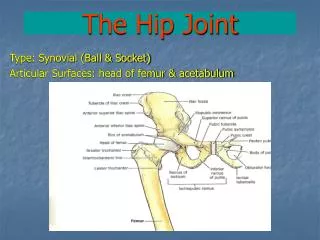
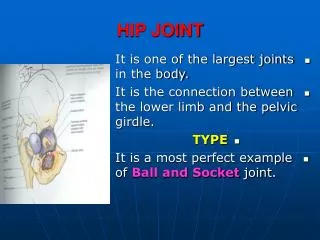
HIP JOINT. ARTICULAR SURFACES. The head of the femur articulates with the acetabulum . The wide superior part of the articular surface is the weight bearing area. So, it is the ilium that bears the weight.

HIP JOINT
E N D
Presentation Transcript
Prof. Saeed Makarem HIP JOINT
ARTICULAR SURFACES • The head of the femur articulates with the acetabulum . • The wide superior part of the articular surface is the weight bearing area. • So, it is the ilium that bears the weight. • The rim of the acetabulum is defective inferiorly at the acetabular notch, which is bridged by the transverse acetabular ligament. Prof. Saeed Makarem
ARTICULAR SURFACES • The head of the femur is covered with hyaline cartilage, except over the fovea or pit, to which the ligament of the head of the femur is attached. • More than half of the femoral head is contained within the acetabulum. • The articular or lunate surface of the acetabulum is horseshoe-shaped. • The acetabulum has a centrally located nonarticularacetabular fossa, which is occupied by a fat that is covered with synovial membrane. Prof. Saeed Makarem
acetabular labrum • The depth of the acetabulum is increased by the fibrocartilaginous rim (acetabular labrum) .It is attached to the rim of the acetabulum and to the transverse acetabular ligament. • The labrum deepens the socket for the femoral head and its free edge clasps the head beyond its widest diameter. • This helps to hold it firmly in the acetabulum (i.e., preventing its dislocation). Type of joint: Synovial ball and socket Prof. Saeed Makarem
FIBROUS CAPSULE • It is strong and dense. • Proximally, it is attached to the edge of the acetabulum, outside the acetabular labrum, and to the transverse acetabular ligament. • Distally, it is attached to the neck of the femur as follows: • anteriorly to the intertrochanteric line and • posteriorly to the neck proximal to the intertrochanteric crest. Prof. Saeed Makarem
SYNOVIAL MEMBRANE Lines the fibrous capsule • It covers the portion of the neck of the femur that lies within the joint capsule. • It surrounds the ligament of head of the femur and covers the pad of fat of acetabular fossa. • A pouch of synovial membrane frequently protrudes through a gap in the anterior wall of the capsule, between the pubofemoral and iliofemoral ligaments, and forms the psoas bursa beneath the psoas tendon. Prof. Saeed Makarem
Ligaments Iliofemoral: • anterior • Triangular Y- shaped • It’s apex attached to the ilium (AIIS). • It’s base forms 2 bands which attached to the upper & lower parts of the intertrochanteric line • Function: It prevents hyperextension of the joint.
ISCHIOFEMORAL LIGAMENT • It is spiral in shape. • It arises from the ischial portion of the acetabular rim and spirals infero- laterally to the neck of the femur, • It reinforces the capsule of the hip joint posteriorly and limits extension of the hip. Prof. Saeed Makarem
PUBOFEMORAL LIGAMENT • Triangular in shape. • It s base is attached to superior pubic ramus. • Its apex is attached to intertrochanteric line. • It limits abduction and extension of the hip joint Prof. Saeed Makarem
TRANSVERSE ACETABULAR LIGAMENT • The transverse acetabular ligament bridges the acetabular notch. • The ligament converts the notch into a tunnel through which the blood vessels and nerves enter the joint. Prof. Saeed Makarem
LIGAMENT OF THE HEAD OF THE FEMUR • Intracapsular ligament, about 3.5 cm long, • It is flat and triangular in shape. • It's wide end is attached to the margins of the acetabular notch and to the transverse acetabular ligament, and its narrow end is attached to the femoral fovea. • It contains a smallartery to the head of the femur, which is a branch of the obturator artery. • It is surrounded by a sleeve of synovial membrane. • This ligament is stretched when the flexed thigh is adducted or laterally rotated. • It is weak and appears to be of little importance in support of the hip joint. Prof. Saeed Makarem
NERVE SUPPLY The articular nerves are derived from: • • The femoral nerve via the nerve to the rectus femoris . • • The obturator nerve via its anterior division; • • The sciatic nerve via the nerve to the quadratus femoris . • • The superior gluteal nerve. Prof. Saeed Makarem
BLOOD SUPPLY The articular arteries are branches of • Medial and lateral circumflex femoral arteries, • Posterior division of the obturator artery (the artery to the head of the femur), • Deep division of the superior gluteal artery, and • The inferior gluteal artery. Prof. Saeed Makarem
IMPORTANT RELATIONS • Anteriorly: • Iliopsoas, • Pectineus, • Rectus femoris. • Iliopsoas and pectineus separate the femoral vessels and nerve from the joint. • Posteriorly: • Obturator internus, • Gemelli, • Quadratus femoris • These muscles separate the joint from the sciatic nerve. • Superiorly: • Piriformis. • gluteus minimus. • Inferiorly: • Obturator externus Prof. Saeed Makarem
Trendelenburg’s Sign Standing on one foot needs: 1- Intact gluteus medius & minimus. 2- Intact superior gluteal nerve. 3- Intact neck of femur 4- Normal angle of neck of the femur. 5- Head of femur must be located within the acetabulum. Pelvis sinks downward on the opposite (unsupported side)
Shenton’s Line The superior margin of obturator foramen forms a smooth continuous curve with the inferior margin of the neck of femur.
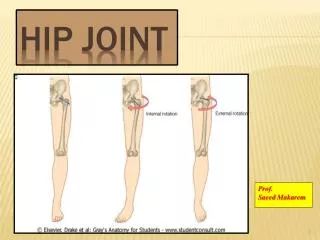
Prof. Saeed Makarem MOVEMENTS • Flexion is performed by the: • iliopsoas, • rectus femoris, • sartorius, and also by the • adductor muscles. • Extension (a backward movement of the flexed thigh) is performed by the: • gluteus maximus and the • hamstring muscles. • Abduction is performed by the: • gluteus medius and minimus • assisted by the sartorius, tensor fasciae lata, and piriformis. • Adduction is performed by the: • adductor longus and brevis and the • adductor fibers of the adductor magnus. • These muscles are assisted by the pectineus and the gracilis. • Lateral rotation is performed by the: • piriformis, • obturator internus and externus, • superior and inferior gemelli, and • quadratus femoris, • assisted by the gluteus maximus. • Medial rotation is performed by the • anterior fibers of gluteus medius and gluteus minimus and the • tensor fasciae latae. • Circumduction is a combination of the above movements. • It should be remembered that the extensor group of muscles is more powerful than the flexor group, and that the lateral rotators are more powerful than the medial rotators.
The hip joint has a wide range of movement, but less than the shoulder . Some of the movement has been sacrificed in order to provide stability. The strength of the joint depends largely on the shape of the bones and on the very strong ligaments. When the knee is flexed, flexion is limited by the anterior surface of the thigh coming into contact with the anterior abdominal wall. When the knee is extended, flexion is limited by the tension of the hamstring muscles. Extension, which is the movement of the flexed thigh backward to the anatomical position, is limited by the tension of the 3 extra-capsular ligament ( Iliofemoral, pubofemoral, and ischiofemoral ) Abduction is limited by the tension of the pubofemoral ligament, and adduction is limited by contact with the opposite limb and by the tension in the ligament of the head of the femur. Lateral rotation is limited by the tension in the iliofemoral and pubofemoral ligaments, and medial rotation is limited by the ischiofemoral ligament. Prof. Saeed Makarem MOVEMENTS