Comprehensive Assessment of SI Joint Dysfunction in a Postnatal Female Patient
This case study discusses a 30-year-old female client, four weeks postpartum, who presents with sacroiliac joint pain affecting her daily activities. Despite prior treatments for pelvic alignment, she experiences persistent symptoms during various movements. The study employs multiple clinical tests, including the General Scan, Leg Length Difference Test, Kinetic Test, and Thomas Test, to assess the functionality and limitations of the pelvic region. The findings indicate potential joint lesions and suggest targeted therapeutic exercises to alleviate pain and improve mobility.

Comprehensive Assessment of SI Joint Dysfunction in a Postnatal Female Patient
E N D
Presentation Transcript
Back and Pelvis Lab 4 Case Study #2 Group #6
IntroductionCase Study Client • 30 year old female (4 weeks post natal) • Experiences pain in her SI region during walking gait, sitting, standing, sleeping • Difficulty with lifting • Previously treated for sacral displacement and pelvic re-alignment for last 4 weeks • Regained range through passive walking program and anti inflammatory drugs • Client is a pronator with knee problems due to foot malfunction • Client has medium lumbar lordosis and slight scoliotic spine • Client experienced low back pain prior to pregnancy, however not SI joint related
General ScanStanding Forward Bend Test • Patient stands with feet shoulder width apart • Clinician faces patients back, places thumbs on patients PSIS and hands on iliac crest • Clinician instructs patient to bend forward • If SI joint is normal, clinicians thumbs will move inferiorly as patient bends forward • If lesion is present, thumb on affected side will either move upward or not move at all • Test identifies side of lesion, however does not identify type of lesion
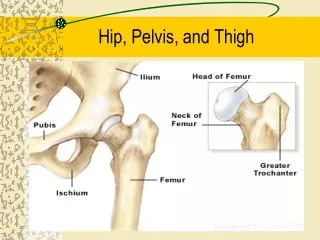
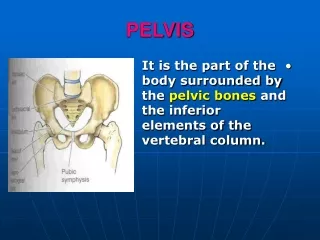
Possible Limitations • Possible limitations that could affect movement of the pelvic region include damage to: • sacrotuberous, sacroiliac, and sacrospinous ligaments • Muslces that could limit movement of the pelvic region include: • Hip flexors (ilio psoas, rectus femoris), hip extensors (gluteus maximus, biceps femoris)
General ScanLeg Length Difference Test • Clinicians instructs patient to lie supine on table with patient’s arms by their side • Clinician instructs patient to flex both legs at hips and knees then move legs to full extension in supine position • Clinician lightly shakes patient’s legs at feet to ensure relaxation of patient • Clinician observes spine of patient to see if spine is perpendicular to ASIS • Clinician places both medial malleoli’s together and takes note of differences in leg length • *A leg length discrepancy does not necessarily entail that the patient has a lesion in their SI joint. This test should be used in conjuction with other SI tests to ensure complete accuracy
General ScanKinetic Test • Patient stands with her back to clinician • To evaluate the left side of patient, the clinician places one thumb on the patients left PSIS and other thumb on the mid sacrum of the same side • The clinician instructs the patient to lift her left knee toward her chest • If the SI is normal the clinicians left thumb on affected side will move inferiorly • If a lesion is present, clinicians left thumb will stay at same point or move superiorly • Clinician then tests patient’s right side by instructing patient to flex right leg while their hands remain in their original position • Clinician then repeats the same test on the right side with their thumb on patient’s right PSIS and other thumb on the mid sacrum same side
Thomas Test • Part 1(PROM) • Patient lies supine on examination table • Spine is square to ASIS • Clinician stabilizes patient’s back by supporting lumbar spine with hand • Clinician flexes a leg up towards patient’s chest • Note when lumbar lordosis flattens and the patients back touches your hand • Once lordosis is flattened continue flexion at hip until end point • *120 degrees is normal • Goniometer is used to measure and record range of motion at hip • Repeat on other side
Thomas Test Con’t • Part 2 (AROM) • Patient holds one leg up by their chest while extending their other leg • Watch for the patient rocking forward/lifting of the thoracic spine or arching/reformation of the lumbar lordosis • Either rocking or arching of the back are evidence that the patient has a contracture • Extent of the contracture can be measured as the angle created between the leg and table • Repeat for the other side
Functional Test 1)Lifting box from different levels a) Lift box off chair on to table: • To begin patient stands close to table • Patient then moves farther away from table when they feel more comfortable • One foot slightly in front of the other and feet are shoulder width apart for balance • Lifting is done with legs not back (flex at knees) b) Lift box from floor to table: • Repeat the steps mentioned above
Functional Test Con’t 2)Sit and tie shoes then stand up: • Patient starts standing then moves to a seated position • Patient then leans forward to tie shoes on one foot, then ties shoes on other foot • Next patient stands up • Clinician watches if patient: • Uses hands to get off chair • Rocks back and forth for momentum • Adjusts leg width or pushes off with toes of non-tying foot • Wraps leg around chair
References • Hoppenfield, JA (1934). Physical Examination of Spine and Extremities. New York : Appleton-Century-Crofts. • Houglum, Peggy A. (n.d.). Therapeutic Exercise for Musculoskeletal Injuries, 2nd ed. • Oatis, Carol A. (2004). Kinesiology: The Mechanics & Pathomechanics of Human Movement. Pennsylvania: Lippincott, Williams & Wilkins