Download
1 / 30
310 likes | 351 Vues
Carpal Tunnel Syndrome (CTS) is a common hand and wrist condition characterized by pain, numbness, and weakness in the median nerve distribution. Learn about anatomy, causes, symptoms, and diagnostic tests for CTS.

E N D
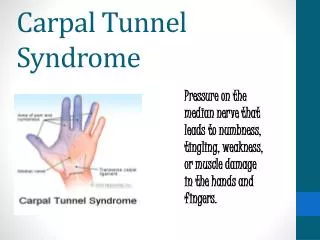
HAND AND WRIST DISEASES Carpal Tunnel Syndrome Carpal tunnel syndrome (CTS) is the most commonly diagnosed and treated entrapment neuropathy. The syndrome is characterized by pain, paresthesia, and weakness in the median nerve distribution of the hand. Surgical and nonsurgical treatments exist that can produce excellent outcomes for patients.
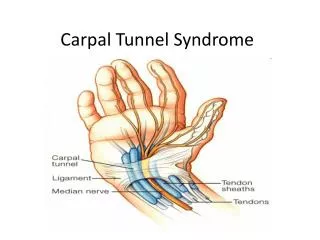
RELEVANT ANATOMY The carpal canal is a fibro-osseous tunnel at the wrist through which 9 flexor tendons and the median nerve pass. The carpal bones define the dorsal aspect of the carpal canal and are shaped in a concave arch. The palmar aspect of the carpal canal is defined by the flexor retinaculum, which bridges the 2 sides of the carpal arch. Intrinsic and extrinsic ligaments of the wrist and hand further stabilize the carpal bones. The carpal canal is narrowest at the level of the hook of the hamate, where the canal averages 20 mm in width.
Etiology • 1-local median nerve compression at the wrist, with ischemia and impaired axonal transport of the median nerve across the wrist. Compression results from elevated pressures within the carpal canal.Elevated pressures can develop within the carpal canal even though the canal is not a separate, closed compartment within the upper extremity. Direct pressure or a space-occupying lesion within the carpal canal can increase pressure on the median nerve and produce CTS. Fracture callus, osteophytes, anomalous muscle bodies, tumors, hypertrophic synovium, and infection, as well as gout and other inflammatory conditions, can produce increased pressure within the carpal canal. Extremes of wrist flexion and extension also elevate pressure within the carpal canal. • 2-systemicconditions are strongly associated with CTS. These conditions may directly or indirectly affect microcirculation, pressure thresholds for nerve conduction, nerve cell body synthesis, and axon transport or interstitial fluid pressures. Perturbations in the endocrine system, as observed in individuals with diabetes and hypothyroidism and in women who are pregnant, are linked to CTS. Conditions affecting metabolism (eg, alcoholism, renal failure with hemodialysis, mucopolysaccharidoses
Clinical • Acute CTS can develop following a major trauma to the upper extremity (typically a distal radius fracture), a carpal dislocation, or a crush injury. Swelling, pain, and paresthesia in the median nerve distribution of the hand (palmar and radial) are observed. In the more common idiopathic or chronic CTS, symptoms are more gradual in onset. Pain and paresthesia in the median nerve distribution of the hand are common. Symptoms are often worse at night and can wake a patient from sleep. As the condition worsens, daytime paresthesia becomes common and is often aggravated by daily activities, such as driving, combing the hair, and holding a book or phone. Weakness can be present. With long-standing or severe cases of CTS, thenar atrophy is frequently observed.Because of the motor and sensory disturbances, manual dexterity is diminished, and difficulty with such daily activities as buttoning clothes and holding small objects is often encountered. Pain and paresthesia can also occur proximally in the forearm, elbow, shoulder, and neck in up to one third of patients(double crush phenomena). Pain and paresthesia in the hand are not always isolated to median nerve distribution but can involve the ulnar aspect or the entire hand.
Provocative tests :- • Phalen wrist flexion test- The patient's elbows are placed on a table, with the forearms perpendicular to the table and the wrists flexed. This position is held for 60 seconds. The test is positive if numbness or paresthesia develops in radial-sided digits. • Tinel test - The examiner taps along the course of the median nerve on the volar aspect of the wrist. The test is positive if paresthesia is elicited in the median nerve distribution. • Carpal compression test - Direct application of pressure of 150 mm Hg or even pressure from both thumbs of the examiner is exerted on the patient's carpal canal and is maintained for 30 seconds. The test is positive if pain, numbness, or paresthesia develops in the radial-sided digits.
Electrophysiologic diagnostic studies –: • 1-Nerve conduction:-Median motor and sensory latencies, as well as conduction velocities, are measured across the wrist. A sensory latency of greater than 3.5 milliseconds or a motor latency of greater than 4.5 milliseconds is considered an abnormal finding. • 2- Electromyography :-This study must be performed with a clinical differential diagnosis in mind; the abductor pollicis brevis is the key muscle to evaluate. Positive findings in persons with CTS include sharp waves, fibrillation potentials, and increased insertional activity.When interpreting electrophysiologic studies, remembering that CTS is a clinical diagnosis is important. CTS is a constellation of signs and symptoms caused by the compression and slowing of the median nerve at the wrist. Electrodiagnostic studies should not be used independently in making a diagnosis.
TREATMENT :-Medical Therapy: • Steroid injection and wrist splintinghave been used effectively in patients with milder symptoms. A study reported complete relief of all symptoms in 76% of hands at 6 weeks after treatment, but more than 12 months after treatment, the proportion of hands experiencing complete relief deteriorated to only 22%. Similar positive results have been reported with steroid injection alone in a double-blind, placebo-controlled trial. Other nonoperative treatments have been proposed, but they have not been studied as rigorously; they include nonsteroidal anti-inflammatory drugs (NSAIDs), vitamins (B complex), workstation redesign, ergonomic tool modification, acupuncture. • Surgical Therapy: • Open and endoscopic surgical techniqueshave been described for treatment of CTS. Both operative techniques are effective for the treatment of chronic CTS. Potential benefits of the endoscopic technique, including a more rapid functional recovery, have to be weighed against the technique's increased cost and higher complication rate. The reliability of and good visualization provided by the open technique continue to make it the preferred operation for many hand surgeons. Open release with an extended surgical incision is recommended for acute CTS.
Dupuytren Contracture • Dupuytren contracture, a disease of the palmar fascia, results in the thickening and shortening of fibrous bands in the hands and fingers. This disease entity belongs to the group of fibromatoses that include plantar fibromatosis (Ledderhose disease), penile fibromatosis (Peyronie disease), and fibromatosis of the dorsal proximal interphalangeal (PIP) joints (Garrod nodes or knuckle pads). • Race, Sex, and Genetics:-The incidence of Dupuytren contracture is highest in Caucasians, historically those of Celtic descent. The disease affects men 7-15 times more often than it does women. Dupuytren disease has long been known to be transmitted in an autosomal dominant fashion with variable penetrance. Neumuller et al (1994) demonstrated an increased relative risk of 2.94 for individuals who express human leukocyte antigen (HLA)-DR3.
Dupuytren disease is an autosomal dominant fibroproliferative disease with variable penetrance. • Associated conditions:-The incidence of Dupuytren disease also increases with concurrent patient clinical conditions or factors such as diabetes, smoking, chronic alcoholism, seizures, and infection . HIV infection,repetitive manual trauma,Age and family history, younger individuals with a positive family history for the Dupuytren disease have been reported, although the disease most often affects people older than 50 years. (Rheumatoid arthritis is associated with a decreased incidence of Dupuytren contracture).
Clinical • The typical patient with Dupuytren disease is aged 50 years or older and presents with a palmar nodule and cord adherent to the skin, as well as with a flexion contracture ,Dupuytren disease must be distinguished from several other conditions that affect the hand, including trigger finger, stenosing tenosynovitis, a ganglion cyst, or a soft-tissue mass
Medical therapy • In the past, nonsurgical approaches to Dupuytren contractures such as splinting, irradiation, ultrasonography, dimethylsulfoxide, vitamin E therapy, and allopurinol treatment were shown to be ineffective. Steroids produced only temporary therapeutic effects, and their use has been debated in the literature. Future nonoperative therapies include the use of calcium channel blockers or gamma-interferon, skeletal traction, and percutaneous needle fasciotomy, with the last of these showing the most promise with minimal adverse effects. • Surgical therapy • Although the option for surgery in Dupuytren disease is considered on a case-by-case basis, guidelines for the timing of surgery exist. In general, surgery should be performed on an affected MCP joint if the contracture is 30° or greater. Such contractures most likely cause some debilitation for the patient. Usually, a limited fasciectomy of the pretendinous cord is sufficient to establish normal function in the MCP joint and no recurrence with a full-thickness skin graft in dermatofasciectomy.
` Hand Infections • 1-Acute paronychia involves the soft tissue around the fingernail and usually results from the inoculation of bacteria (most commonly Staphylococcus aureus) into the paronychia tissue from nail trauma or nail manipulation. • 2-Chronic paronychia usually is caused by Candida albicans and occurs most commonly from chronic immersion in water (as in dishwashers), previous trauma, or nail defects. • 3-A felon is a subcutaneous abscess over the distal pulp of a digit or thumb. Felons usually result from a penetrating injury. The pulp contains multiple compartments separated by fibrous septa that make infections in this area complex. • 4-Deep-space infections in the hands are possible; the 2 deep spaces in the palm are the midpalmar space and the thenar space. Infections in these areas usually result from injuries such as bites or puncture wounds. These infections may cause cellulitis, fluctuance, and/or pain. In addition, the second, third, and fourth web spaces are potential sites for infection. Web-space infections can spread from the palmar subfascial space in a dorsal direction, forming what is commonly referred to as a "collar button abscess." On examination, patients typically have pain, swelling, and fluctuance on the palmar or dorsal web-space surface. • 5-Flexor tenosynovitis is a potentially devastating infection that can result in significant scarring of the flexor tendon sheath with resultant compromise in hand function. These infections usually are caused by a penetrating injury (eg, bite, puncture wound). • 6-Septic arthritis usually results as a sequela after open skeletal trauma or from a bite wound. Patients with inflammatory arthritis are at increased risk for joint-space infections. Tenderness and swelling of the joint are signs of potential infection. Puncture wounds over the joint should suggest potential septic arthritis. The differential diagnosis includes gout, psoriatic arthritis flare, and systemic lupus erythematosus. Staphylococci and streptococci are most commonly isolated in septic joint cultures. • 7-Osteomyelitis can occur from an acute event, such as a penetrating wound or open fracture, or as a late sequela of a fracture or other surgery. Patients with a history of diabetes or other immunocompromising conditions are at higher risk for osteomyelitis. Diagnosis of this condition is based on the signs seen with other infections: cellulitis, warmth, and tenderness. In addition, recurrent infections in the same location may be a sign of infection of the underlying bone. Laboratory studies and radiographs can assist in making the appropriate diagnosis . The treatment consists of debridement of the devitalized bone, as well as antibiotics, usually a prolonged course of 6 weeks. • 8-Herpetic whitlow is a viral infection that is caused by the herpes simplex virus and that may resemble a felon or paronychia. These infections usually occur in medical or dental personnel. History is an important clue to the diagnosis. The patient first notices pain, then erythema before the development of the herpetic vesicle.
Clinical • A thorough history of a hand infection includes determination of the onset, duration, any recent trauma, and any systemic symptoms (eg, fever, chills). Most patients present with a 2- to 3-day history of cellulitis and swelling. • The physical examination should include examination of the hand, with particular attention to cellulitis, lymphangitis, areas of fluctuance, range of motion, foreign bodies, and the presence or absence of Kanavel signs.The 4 Kanavel signs are used to differentiate between infectious tenosynovitis and a superficial or localized abscess. In the presence of infectious tenosynovitis, the signs include intense pain, flexion posture, uniform swelling, and percussion tenderness.
Medical therapy • A few important guidelines assist in the management of hand infections. First, cellulitis must be treated with antibiotics. Most hand infections are caused by Staph aureus,and therefore, a first-generation cephalosporin (eg, cephalexin) is usually the first drug of choice. However, the potential exists for infections with different organisms. In fact, an increase in the incidence of community-acquired methicillin-resistant staphylococcal (MRSA) infections has been reported. • Animal bites require bacterial coverage that is particular to the offending animal. Human bites require coverage for Eikenella corrodens; penicillin and a first-generation cephalosporin are appropriate choices in these cases. Cat bites require coverage for Pasteurella multocid; appropriate antibiotics include IV ampicillin/sulbactam or oral amoxicillin clavulanate. • Usually, oral antibiotics are sufficient as initial treatment. Many medical professionals recommend an initial, limited wound irrigation in the emergency department or in the outpatient clinic. Consider IV antibiotics in patients in whom cellulitis fails to resolve with oral antibiotics. In all cases, the final antibiotic coverage should be guided by culture and sensitivity results. Patients with a history of immunocompromise (including those with diabetes) should initially be treated with IV antibiotics. • Fungal infections can occur in or under the skin. Cutaneous fungal infections, or tinea, are treated with topical agents such as miconazole or clotrimazole. The most common subcutaneous infection is sporotrichosis; this condition can appear with an ulcerative lesion, along with lymphadenopathy. Gardeners are most commonly infected. Oral itraconazole for 3-6 months is the current recommended course of treatment. Fungal abscesses or disseminated fungal infections can occur and are usually found in immunocompromised patients. • Surgical therapy • As a rule, all abscess cavities must be drained. Antibiotics alone are not effective in treating pus. If the patient does not improve with antibiotics, suspect undrained pus or a foreign body. Immunocompromised patients should always receive IV antibiotics.
Lab Studies • Complete blood cell (CBC) count: An elevated white blood cell count can indicate the presence of infection. • Prothrombin time (PT) and activated partial thromboplastin time (aPTT): Obtain these tests before surgical treatment in patients who are receiving long-term anticoagulant therapy. • Glucose level: Check glucose levels in all patients with a history of diabetes. In those patients with active infections, blood-glucose levels are often elevated and difficult to control. Furthermore, blood-glucose control is important for wound healing. It is also important to check the glucose levels of any patient who has a history of frequent or particularly severe infections to rule out occult diabetes. • Erythrocyte sedimentation rate (ESRand CRP): are elevated in cases of septic arthritis and osteomyelitis. • If there is a clinical suspicion of septic arthritis, a joint aspirate should be sent for Gram staining, culturing, and sensitivity testing. In addition, cell count assessment, glucose and protein level determinations, and crystal analysis help in distinguishing between an infected joint and a joint with inflammatory arthritis or gout/pseudogout. • Imaging Studies • Plain radiographs (3 views of the hand) are important to rule out the presence of foreign bodies, fractures, and subcutaneous air, which could indicate gas gangrene or acute or chronic osteomyelitis. • Magnetic resonance imaging (MRI) may be helpful for assessing soft-tissue abscess(es) and osteomyelitis. • Ultrasonography may reveal soft-tissue abscess. • Bone scanning, indium-111 (111In) radionuclide studies, or computed tomography (CT) scanning may be useful for evaluating osteomyelitis.
Ganglion Cyst • Ganglion cysts are the most common soft-tissue tumors of the hand and wrist. They can occur in patients of any age, including children; approximately 15% of ganglion cysts occur in patients younger than 21 years. Seventy percent of ganglion cysts occur in patients between the second and fourth decades of life. Women are affected 3 times as often as men. No predilection exists for the right or left hand, and occupation does not appear to increase the risk of ganglion formation. • Etiology • Uncertainty exists regarding the origin of ganglion cysts. The most widely held physiologic explanation attributes cyst formation to mucoid degeneration of collagen and connective tissues. This theory implies that a ganglion represents a degenerative structure that houses . • A more recent theory, postulated by Angelides, attributes cyst formation to trauma or tissue irritation.Modified synovial cells lining the synovial-capsular interface are stimulated to produce mucin. Mucin dissects along the attached joint ligament and capsule to form capsular ducts, which function as valvelike structures producing lakes. The ducts and lakes of mucin eventually coalesce to form a solitary ganglion cyst.
RELEVANT ANATOMY • A ganglion is a well-circumscribed mucin-filled cyst with a smooth translucent wall that is closely associated with a joint or tendon sheath. Ganglions are usually connected by a stalk to an underlying joint capsule or ligament. They commonly arise from the dorsum of the wrist, where they are specifically associated with the scapholunate ligament of the wrist. Volar wrist ganglions are less common, and many are associated with the scaphotrapezial joint of the wrist. • The location of the radial artery is particularly important in the assessment of volar wrist ganglions because they are often intimately associated with this vessel. Care must be taken to preserve the radial artery during dissection of a volar wrist ganglion because injury to this vessel may potentially compromise circulation to the hand. • Clinical • Although ganglion cysts are generally asymptomatic, presenting symptoms may include limitation of motion, pain, paresthesias, and weakness. Ganglions are usually solitary, and they rarely exceed 2 cm in diameter. They can involve almost any joint of the hand and wrist. Dorsal wrist, volar wrist, volar retinacular, and distal interphalangeal ganglion cysts constitute the vast majority of ganglions of the hand and wrist. • Dorsal wrist ganglia occurring over the scapholunate ligament of the wrist represent 60-70% of all ganglia. The volar wrist is the next most common site of occurrence; 20% of all ganglia occur in the volar wrist. The flexor tendon sheath of the fingers, particularly at the level of the A1 pulley, is involved in 10-12% of ganglia.
Imaging Studies • Standard plain radiographs are obtained to evaluate any potential underlying bone or joint abnormality that may explain the symptoms. The cyst itself is rarely visualized. For cases with atypical presentations, and especially occult ganglia, MRI studies have proven to be successful in confirming examination findings. • Medical therapy • The predominant current nonsurgical method of treatment involves aspiration alone,sometimes followed by steroid injection. This is especially successful for tendon sheath ganglions in the hand and digits. Caution should be exercised when performing multiple steroid injections to avoid the complications of skin and fat atrophy and thinning, as well as hypopigmentation. • Surgical therapy • INDICATIONS:- Indications for treatment include limitation of motion, pain, weakness, and paresthesias. Treatment is also indicated if malignancy is a concern or if the patient finds the lesion aesthetically displeasing..Surgical treatment involves total ganglionectomy with removal of a modest portion of the attached capsule.
De Quervain Tenosynovitis • De Quervain tenosynovitis is an entrapment tendinitis of the tendons contained within the first dorsal compartment at the wrist; it causes pain during thumb motion. • Etiology • The tendons of the abductor pollicis longus and the extensor pollicis brevis are tightly secured against the radial styloid by the overlying extensor retinaculum. Any thickening of the tendons from acute or repetitive trauma restrains gliding of the tendons through the sheath. Efforts at thumb motion, especially when combined with radial or ulnar deviation of the wrist, cause pain and perpetuate the inflammation and swelling. • Clinical • Patients note pain resulting from thumb and wrist motion, along with tenderness and thickening at the radial styloid. Crepitation or actual triggering is rarely noted. Patients frequently are mothers of infants aged 6-12 months, and symptoms are often noted in both wrists. Repetitive lifting of the baby as it grows heavier is responsible for friction tendinitis. Day care workers and other persons who repetitively lift infants are frequently affected as well. De Quervain tenosynovitis can also develop in individuals who have sustained a direct blow to the area of the first dorsal compartment. • Examination • The first dorsal compartment over the radial styloid becomes thickened and feels bone hard; the area becomes tender. Usually, the compartment's thickening so distorts the sparsely padded skin in this area that a visible fusiform mass is created. The Finkelstein test (consisting of flexion of the thumb across the palm and then ulnar deviation of the wrist) causes sharp pain at the first dorsal compartment .Tenderness is absent over the muscle bellies proximal to the first dorsal compartment. Tenderness and pain on axial loading are absent at the carpometacarpal (CMC) joint unless the patient has arthritis in that joint.
Medical therapy • Splinting of the thumb and wrist relieves symptoms, but most patients find the loss of the thumb for functional activities too restrictive and do not consistently wear the splints. Injection of corticosteroid into the sheath of the first dorsal compartment reduces tendon thickening and inflammation. A dose of 0.5 mL of 1% plain Xylocaine and 0.5 mL of a long-acting corticosteroid preparation can be injected either sequentially or simultaneously. One injection permanently relieves symptoms in roughly 50% of patients. A second injection given at least a month later permanently relieves symptoms in another 40-45% of patients. • Surgical therapy • If injection therapy fails, surgical release of the first dorsal compartment relieves the entrapment.