Download
1 / 24
771 likes | 4.65k Vues
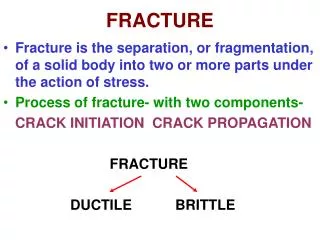
SUPRACONDYLAR FRACTURE. BY : DR SANJEEV. Fig :. SUPRACONDYLAR FRACTURE. Fig :. SUPRACONDYLAR FRACTURE. Supracondylar fracture (Malgaigne`s fracture). Mechanism of injury : Fall on an outstretched hand with hyperextension at the elbow with abduction or adduction , with hand dorsiflexed.

E N D
SUPRACONDYLAR FRACTURE BY : DR SANJEEV
Fig : • SUPRACONDYLAR FRACTURE
Fig : • SUPRACONDYLAR FRACTURE
Supracondylar fracture (Malgaigne`s fracture) • Mechanism of injury : • Fall on an outstretched hand with hyperextension at the elbow with abduction or adduction , with hand dorsiflexed
Classification • Flexion type (2.3 %) • Extension type (97.3 %) : -displaced and undisplaced. • Clinical features : • Pain and swelling – gross • S –shaped deformity of the upper arm is obvious • Loss of both passive and active movements of the elbow • pseudoparalysis
Gartlands classification (in children) • Type 1 :undisplaced • Type 2 :displaced , but posterior cortex is intact • Type 3 : displaced , but no intact posterior cortex.
Fig : • Type 2 : displaced but posterior cortex is intact
Fig : • Type 3 : SUPRACONDYLAR FRACTURE
Clinical signs : • Arm is short , forearm is normal in length • Gross swelling , and tenderness • Crepitus – present • S – shaped deformity • Dimple sign
Radiology • X- ray of the elbow : • A P view • Lateral view
Fig : A P view • Baumann`s angle : angle between the horizontal line of the elbow and the line drawn through the lateral epiphysis and the long axsis of the arm.(normally less than 5 degree
Cont.. • Angle between the long axis of humerus and the transverse of the elbow is normally 90 degree - less than 90 degree suggest cubitus valgus - greater than 90 degree suggests cubitus varus.
Fig :lateral view • Anterior humeral line:a line drawn along the anterior border or distal humeral shaft passes through the middle 1/ 3rd of capitulum. if it passes through anterior 1/3rd , it indicates posterior displacement of the distal fragment.
MANAGEMENT Undisplaced fracture :- - POP slab for 3 weeks with elbow in flexion Displaced fracture : • Closed reduction • Traction • Open reduction • Elbow is immobilised at least for 3 weeks • Pins or casts are removed after 3 weeks • Active exercise.
Complication Neurological : • Radial nerve (commonly ) • Median nerve • Ulnar nerve Vascular : • Brachial artery Cosmetic abnormalities: • Cubitus varus (gunstock elbow)
Complication : • Fig :
Fig : • SUPRACONDYLAR FRACTURE
Fig : • SUPRACONDYLAR FRACTURE
Fig : • Type 2 : displaced but posterior cortex is intact
Fig : • Anterior humeral line: if it passes through anterior 1/3rd , it indicates poterior displacement of the distal fragment.
Fig : A P view • Baumann`s angle : angle between the horizontal line of the elbow and the line drawn through the lateral epiphysis and the long axsis of the arm.(normally less than 5 degree
Complication : • Fig :
Fig : • SUPRACONDYLAR FRACTURE
Fig : • SUPRACONDYLAR FRACTURE