Download
1 / 27
280 likes | 1.51k Vues
Case report - W.H.. 76 yo M with past medical history of BPH and melanoma and known diverticulosis Transferred from an outside hospital with lower gastrointestinal bleedingTransfused 5U PRBC at outside hospital (Hct 26?35)Outside hospital colonoscopy - diverticulosis with no active bleeding; EGD - no pathology.

E N D
1. Angiographic embolization for the treatment of lower gastrointestinal bleeding Donald Baril
Team IV Conference
July 9, 2004
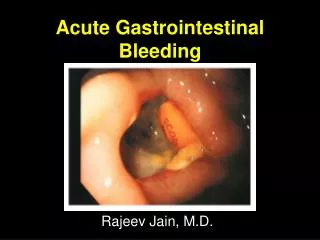
2. Case report - W.H. 76 yo M with past medical history of BPH and melanoma and known diverticulosis
Transferred from an outside hospital with lower gastrointestinal bleeding
Transfused 5U PRBC at outside hospital (Hct 26?35)
Outside hospital colonoscopy - diverticulosis with no active bleeding; EGD - no pathology
3. Case report - W.H. Transferred to SICU
Hemodynamically stable
Continued to have hematochezia with dropping hematocrit (35 ? 22) and was transfused an additional 9U PRBC over the following 3 days
Bleeding scan localized source to the cecum and ascending colon
Proceeded to angiography and embolization
4. SMA angiogram
5. Selective SMA and ileocolic angiogram
6. Selective ileocolic angiogram with coil deployment
7. Post-embolization angiogram
8. Case report - W.H. Tolerated regular diet
Hematocrit remained stable
Discharged home on post-procedure day #3
9. Lower gastrointestinal bleeding Annual incidence of 25 per 100,000 patients
Gastrointestinal bleeding accounts for 2% of all hospital admissions
Lower gastrointestinal bleeds account for approximately � of all patients admitted with gastrointestinal bleeding
Incidence of bleeding increases with age
Bleeding spontaneously ceases in 80% of cases
Mortality rates of 10-15%
10. Etiology of lower gastrointestinal bleeding Adolescents and children
Inflammatory bowel disease, polyps, Meckel�s diverticulum
Adults < 60
Diverticular disease, neoplasms, inflammatory bowel disease
Adults > 60
Diverticular disease, angiodysplasia, neoplasms
11. Etiology of lower gastrointestinal bleeding Diverticular disease - most likely cause of LGIH in adults 30 and 40 %
Arteriovenous malformations 1 to 4 percent
Diverticular disease - most likely cause of LGIH in adults 30 and 40 %
Arteriovenous malformations 1 to 4 percent
12. Diverticular disease Present in 66% of patients older than 80 years
Diverticuli form at the site where the vasa recta penetrate the muscular wall of the colon
10-20% of patients with diverticular disease will experience bleeding
Right-sided diverticli have a higher incidence of bleeding
13. Diagnostic/Therapeutic options - Colonoscopy May be therapeutic (cauterization, injection of vasoconstricting agents, placement of hemostatic clips)
Complete evaluation requires bowel preparation
Often limited visualization in the presence of ongoing bleeding
14. Diagnostic options - Tagged red blood cell scanning Technetium-99 labeled red blood cell scanning detects 90% of active gastrointestinal bleeds
May detect bleeding at a rate of 0.1ml/min
Scanning is performed continuously over 2 hours
Radiotracer remains active for 48 hours
Should not be used alone to determine the location of a segmental resection
If positive, patient should proceed to angiography
15. Tagged red blood cell scanning
16. Angiography and embolization Initially attempted in the mid-1970s
During the 1980s, selective vasopressin infusion became the endovascular therapy of choice
Re-emerged as a leading therapy in the early 1990s with the advent of microcatheters, torqueable guidewires and high-resolution angiographic equipment
Currently, no prospective studies to evaluate the outcomes of angiographic embolization and no consensus on optimal post-embolization care
Angiography remains the gold standard for the diagnosis of lower gastrointestinal bleeding (detects 0.5-1mL/min)
17. Mechanism of embolization Goal of embolization is to decrease perfusion pressure enough to stop hemorrhage but not to a level of complete devascularization
Embolization materials decrease perfusion pressure and induce local vasospasm
Allows for the patient to more effectively form clot
Superselective placement less important in the upper gastrointestinal tract given the rich collateral supply
18. Typical arterial access via femoral or brachial artery
5 French catheter is used to select a first-order vessel (IMA or SMA)
Microcatheter (2.5 to 3 French) may then be advanced to the marginal artery or vasa recta?�superselective catheterization� Angiographic embolization
19. Embolic agents Gelfoam
Sterile gelatin sponge
Insouble in water, pourous
Temporary and allows for vessel recanalization in days to weeks
Polyvinyl alcohol particles
Incites intraluminal thrombosis with an associated inflammatory reaction
Gross appearance similar to sand
Microcoils
Constructed from platinum
Biocompatible but highly thrombogenic
20. Microcoils
21. Embolization outcomes Overall success rates of 70 to 100%
Ischemic complications range from 0 to 20%
Bowel necrosis requiring surgical intervention is less than 10%
22. Embolization outcomes - DeBarros et al. DCR 2002 27 patients: Diverticulosis - 22, AVM - 5
100% initial technical success with cessation of bleeding
22.2% rebleeding rate
5/6 patients who rebled underwent surgery
2 patients developed postembolization ischemia; 1 required operative intervention
All patients had follow-up within one year and none demonstrated any evidence of ischemia (including stricture formation) on colonoscopy
23. Embolization outcomes - Kuo et al. JVIR 2003 22 patients: Diverticulosis - 7, Neoplasm - 5
100% initial technical success with cessation of bleeding
14% rebleeding rate
All patients who rebled underwent colonoscopy with subsequent control of the bleeding
1 patient developed postembolization ischemia which was treated conservatively
24. Limitations of superselective embolization Unable to diagnose and treat patients who are not actively bleeding
Target vessel may not be accessible due to atherosclerotic occlusive disease or vasospasm
Bleeding from a surgical anastamosis should be a relative contraindication given the limited collateral blood supply
25. Vasopressin - Past its prime? Vasopressin
Infusion leads to successful cessation of bleeding in 80% of cases
Does not require superselective catheterization
Bowel infarction is extremely rare
Side effects reversible with cessation of infusion
Infusion requires only a single 5 Fr catheter
Requires ICU monitoring
Infusion time may be greater than 24 hours
Rebleeding rates of up to 50%
Side effects include coronary vasoconstriction, arrhythmias, and bowel infarction
26. Control of LGIH with vasopressin
27. Conclusions Angiographic embolization is a relatively safe and effective procedure for patients with LGI bleeding
Hemostasis achieved by angiographic embolization may be definitive therapy and, at least, allows for semi-elective operative resection
Given superselective embolization, the risk of significant post-procedure ischemia is quite low
Unknown if routine immediate post-procedure colonoscopy is of value
Unknown long-term risks for rebleeding