Download
1 / 34
350 likes | 427 Vues
Explore the role of functional connectivity in diseases affecting the brain and nervous system in this comprehensive educational course from the University of Oxford. Learn about the implications of abnormal connectivity in conditions like schizophrenia, Alzheimer's, Parkinson's, and more. Understand the advantages and challenges of using resting-state fMRI to study functional networks and analyze diseases. Gain insights into seed-based and ICA-based approaches in studying conditions such as Parkinson's and Alzheimer's disease.

E N D
ISMRM Educational course – 10th of May 2014 Functional connectivity: Diseases of connectivity Gwenaëlle Douaud FMRIB, University of Oxford
Diseases of connectivity or disconnection? • Lesion/degeneration/synaptic malfunction structural connectivity functional connectivity (e.g., Cabral et al., 2012): • Abnormal functional connectivity in schizophrenia Alzheimer’s Parkinson’s chronic pain depression • Functional connectivity impairment disconnection syndrome, where “damage to the connection results in deficit that is dinstinct both from damage to the target and source regions” (Kleinschmidt & Vuilleumier, 2013) Gerstmann syndrome: acalculia +finger agnosia +left-right disorientation +agraphia Rusconi et al., 2009 ISMRM Educational course – 10th of May 2014
Resting-state fMRI: advantages • Increased signal-to-noise ratio (Fox & Greicius, Review 2010): • - at best, task-related modulation explains 20% of BOLD variance • - spontaneous ongoing activity explains 50-80% of BOLD variance ISMRM Educational course – 10th of May 2014
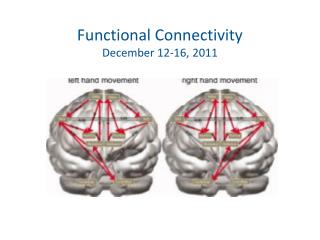
Resting-state fMRI: advantages • Covers the entire repertoire of functional networks used by the brain in “action” • (Smith et al., 2009) RSN: 36 healthy subjects fMRI: ~7,300 maps, ~30,000 subjects ISMRM Educational course – 10th of May 2014
Resting-state fMRI: advantages • Allows for a broader sampling of patient populations asleep, sedated, too impaired for task-based fMRI scanning, etc. Greicius et al., 2008 • Is not confounded by task performance, effort, practice effects, etc. ISMRM Educational course – 10th of May 2014
Resting-state fMRI: inconvenients • “Rest” is a task state in itself, with potential performance differences, rather than differences in the underlying, stable brain organisation (Buckner et al., 2008, 2013) • “Rest” is a task state in itself, with potential performance differences, rather than differences in the underlying, stable brain organisation (Buckner et al., 2008, 2013) Might still reveal some meaningful differences, just need careful interpretation Might still reveal some meaningful differences, just need careful interpretation • More susceptible to movement confounds: • add motion parameters as covariate • use ICA+FIX (automatic denoising using FSL tools: Salimi-Khorshidi et al., 2014, Griffanti et al., 2014) ISMRM Educational course – 10th of May 2014
Resting-state fMRI: inconvenients • Interpretation: • - no causality information (yet) effective functional connectivity • - no easy interpretation what (a change in) + and – correlations mean Smith et al., 2013 ISMRM Educational course – 10th of May 2014
Resting-state fMRI in disease: reviews • Mild cognitive impairment/Alzheimer’s disease: • - Dennis & Thompson, 2014 • - Sheline & Raichle, 2013 • Movement disorders (esp. Parkinson’s disease): • - Poston & Eidelberg, 2012 • Psychiatric disorders (e.g., schizophrenia, ADHD, autism): • - Greicius, 2008 • - Posner et al., 2014 ISMRM Educational course – 10th of May 2014
Resting-state fMRI analysis: seed-based approach in Parkinson’s disease • Seed-based approach - a priori knowledge/hypothesis • Parkinson’s disease: Helmich et al., 2010 ISMRM Educational course – 10th of May 2014
Resting-state fMRI analysis: seed-based approach in Parkinson’s disease • Seed-based approach - a priori knowledge/hypothesis • Parkinson’s disease: Helmich et al., 2010 ISMRM Educational course – 10th of May 2014
Resting-state fMRI analysis: seed-based approach in Parkinson’s disease • Seed-based approach - a priori knowledge/hypothesis • Parkinson’s disease: Helmich et al., 2010 Functional compensation with anterior putamen “taking over” connections to IPC: increased connectivity between IPC and anterior putamen in Parkinson’s was larger for the least-affected side • Very careful study: • - negative control with DMN • - corrected for motion (higher in patients) • - checked for the effect of tremor: no tremor versus tremor spatial map, regressing out muscle activity (electromyography) • Very careful study: • - negative control with DMN • Very careful study: • - negative control with DMN • - corrected for motion (higher in patients) • - checked for the effect of tremor: no tremor versus tremor spatial map, regressing out muscle activity (electromyography) • - checked effect of medication • - checked for grey matter volume differences of seeds and whole-brain VBM • Very careful study: • - negative control with DMN • - corrected for motion (higher in patients) • - checked for the effect of tremor: no tremor versus tremor spatial map, regressing out muscle activity (electromyography) • - checked effect of medication ISMRM Educational course – 10th of May 2014
Resting-state fMRI analysis: ICA-based approach in Alzheimer’s disease • ICA-based approach – more exploratory (though can also be hypothesis-driven) • Alzheimer’s disease: Zamboni et al., 2013 Dual regression for group comparisons ISMRM Educational course – 10th of May 2014
Resting-state fMRI analysis: ICA-based approach in Alzheimer’s disease • ICA-based approach – more exploratory (though can also be hypothesis-driven) • Alzheimer’s disease: Zamboni et al., 2013 ISMRM Educational course – 10th of May 2014
Resting-state fMRI analysis: ICA-based approach in Alzheimer’s disease • ICA-based approach – more exploratory (though can also be hypothesis-driven) • Alzheimer’s disease: Zamboni et al., 2013 • Resting-state fMRI less confounds, task fMRI more interpretable: • “Increased frontal activity during a memory task overlaps with increased frontal connectivity during rest in AD patients, suggesting that residual cognitive ability can be assessed using resting fMRI.” • Very careful study: • - same number of healthy and AD participants for ICA • - negative control with auditory RSN • - corrected for GM volume • - checked for the effect of physiological fluctuations (respiratory + cardiac activity) ISMRM Educational course – 10th of May 2014
Resting-state fMRI analysis: Graph-based approach in schizophrenia • Graph theory – exploratory (though mostly no basal ganglia or cerebellum) • Schizophrenia: van den Heuvel et al., 2013 ISMRM Educational course – 10th of May 2014
Resting-state fMRI analysis: Graph-based approach in schizophrenia • Graph theory – exploratory (though mostly no basal ganglia or cerebellum) • Schizophrenia: van den Heuvel et al., 2013 “Reduced level of rich club interconnectivity in patients with schizophrenia (…), potentially resulting in decreased global communication capacity and altered functional brain dynamics” • Careful study: • - includes basal ganglia • - used Freesurfer parcellation for ROIs (as opposed to AAL) • - replication dataset effects not specific to Rich Club • - but: “This study did not reveal a clear association between clinical metrics of patients and rich club organization” • Careful study: • - includes basal ganglia • - used Freesurfer parcellation for ROIs (as opposed to AAL) ISMRM Educational course – 10th of May 2014
Resting-state fMRI analysis: Multi-modal approach in motor neuron disease • Combining information – diffusion tensor and tractography • Amyotrophic lateral sclerosis: Douaud, Filippini et al., 2011 Increase FC in ALS ISMRM Educational course – 10th of May 2014
Resting-state fMRI analysis: Multi-modal approach in motor neuron disease • Combining information – diffusion tensor and tractography • Amyotrophic lateral sclerosis: Douaud, Filippini et al., 2011 • Careful registration (BBR + VBM) Disease duration ISMRM Educational course – 10th of May 2014
Resting-state fMRI analysis: Multi-modal approach in motor neuron disease • Combining information – diffusion tensor and tractography • Amyotrophic lateral sclerosis: Douaud, Filippini et al., 2011 • Higher functional connectivity not necessarily better • Reconciling lower structural connectivity (SC) with higher functional connectivity? corpus callosum GABAergic interneurons Innocenti, 2009 ISMRM Educational course – 10th of May 2014
Resting-state fMRI analysis: Multi-modal approach in motor neuron disease • Combining information – diffusion tensor and tractography • Amyotrophic lateral sclerosis: Douaud, Filippini et al., 2011 • Low SC + high FC in ALS • = loss of GABA interneurons + FC - GABA ISMRM Educational course – 10th of May 2014
Resting-state fMRI analysis: Multi-modal approach in neurodegenerative diseases • Combining information – grey matter volume/structural covariance • Array of neurodegenerative disorders: Seeley et al., 2009 ISMRM Educational course – 10th of May 2014
Resting-state fMRI analysis: Multi-modal approach in neurodegenerative diseases • Combining information – grey matter volume/structural covariance • Array of neurodegenerative disorders: Seeley et al., 2009 • Dissociable networks for each disease ISMRM Educational course – 10th of May 2014
Variability of results in fcMRI Fox & Greicius, 2010 ISMRM Educational course – 10th of May 2014
Variability of results in fcMRI: some guidelines Parkinson’s: Seeds in the striatum DMN as negative control Alzheimer’s: RSN (ICA) involving frontal areas auditory RSN as negative control Fox & Greicius, 2010 ISMRM Educational course – 10th of May 2014
Variability of results in fcMRI: some guidelines + careful registration Fox & Greicius, 2010 ISMRM Educational course – 10th of May 2014
Variability of results in fcMRI: some guidelines + careful registration Fox & Greicius, 2010 ISMRM Educational course – 10th of May 2014
Variability of results in fcMRI: movement • “Scrub” the data, add motion parameters, or use ICA+FIX Power et al., 2012 ISMRM Educational course – 10th of May 2014
Variability of results in fcMRI: movement • “Scrub” the data, add motion parameters, or use ICA+FIX Salimi-Khorshidi et al., 2014 Griffanti et al., 2014 ISMRM Educational course – 10th of May 2014
Variability of results in fcMRI: some guidelines • Global signal regression, # of ICs etc. Fox & Greicius, 2010 ISMRM Educational course – 10th of May 2014
Variability of results in fcMRI: some guidelines Fox & Greicius, 2010 ISMRM Educational course – 10th of May 2014
Variability of results in fcMRI: stability of networks • Inter-subject variability is higher in higher-order regions (Mueller et al., 2013) ISMRM Educational course – 10th of May 2014
Interpretation of functional connectivity results • Some RSN are more stable than others • Higher not necessarily better • Always check for each contrast what happens in each cluster Absolute values of correlations matter ISMRM Educational course – 10th of May 2014
Interpretation of functional connectivity results • Some RSN are more stable than others • Higher not necessarily better • Always check for each contrast what happens in each cluster It’s the absolute values of correlations that matter • Bear in mind that change in correlations can be observed even in the absence of a change in coupling (Friston, 2011) Changes in correlation between A and B could be caused by a change in correlation elsewhere Changes in correlation could be caused by a change in SNR (e.g., heart rate variability differs between two populations) Changes in correlation could be caused by a change in the amplitude of the fluctuations • Bear in mind that “resting” is to some extent also a task ISMRM Educational course – 10th of May 2014
Special thanks to: FMRIB, University of Oxford - Steve Smith • Eugene Duff • Christian Beckmann • Reza Salimi-Khorshidi • Martin Turner • Giovanna Zamboni • Nicola Filippini • Marina Charquero Ballester THANK YOU FOR YOUR ATTENTION ISMRM Educational course – 10th of May 2014