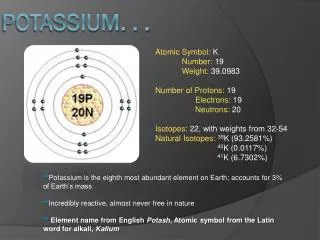
Potassium
Potassium. Emergencies. Joel M. Topf, MD Nephrology Attending. Decreased intake of potassium Alcoholics Anorexia. Transcellular shift of potassium ß-agonists Dobutamine. Renal potassium excretion Diuretics Decreased chloride delivery Hyperaldosteronism. Etiologies of hypokalemia.

Potassium
E N D
Presentation Transcript
Potassium Emergencies Joel M. Topf, MD Nephrology Attending
Decreased intake of potassium • Alcoholics • Anorexia • Transcellular shift of potassium • ß-agonists • Dobutamine • Renal potassium excretion • Diuretics • Decreased chloride delivery • Hyperaldosteronism Etiologies of hypokalemia
EKG findings with hypokalemia • hypokalemia produces EKG changes which are not necessarily related to the K+ level • Flattening of T waves • Increased prominence of U waves (look at V4, 5, 6) • ST depression • Increased prominence of P waves • Inversion of T waves
81-year-old woman develops chest pain during treatment of an asthma exacerbation. • The patient was found to be: • Disoriented • Complaining of stabbing, non-radiating chest pain • Nausea, vomiting, dyspnea • Severe muscle weakness • Potassium of 0.9 mEq/L. • History of taking herbal remedies, including natural licorice. • Licorice contains glycyrrhizic acid
Hypokalemia and Arrhythmias • Norwegians with AMI • N= 1035 • 23 K ≤ 3.0 • 94 K = 3.1-3.5 • 357 K = 3.6-4.0 • 393 K = 4.1-4.5 • 141 K = 4.6=5.1 • 24 K ≥ 5.2 • Results are the incidence of arrhythmias by K level Nordrehaug, JE, Acta Med Scand, Sup. 1981 647, 101-107
Treatment of hypokalemia • Give potassium • Oral is preferred route • 20-40 mEq qd-q6h • KCl is superior to Kphos or K-acetate • IV for patients who are NPO or have dangerously low potassium • Liberal use of K sparing diuretics • Check and correct Mg deficiency
How much K to give • Altered cellular distribution • No total body K deficit so any K given will need to be excreted after the maldistrib-ution is rectified • A compilation of 7 separate metabolic balance studies reveals the following graph Check the Creatinine first
Problems with IV potassium Hyperkalemia Concentrated IV potassium solutions cause phlebitis Dilute IV potassium in saline causes volume overload IV potassium in dextrose cause a release of insulin lowering plasma potassium
Treatment of hypokalemia: IV KCl • N = 40 ICU patients with arterial lines and hypokalemia. • Patients given 20 mmol of KCl in 100 mL • Pre-infusion K = 2.9 • 26 central vein • 14 peripheral • Continuous EKG monitoring in 31 and pre and post 12 lead EKG in all 40. Kruse, JA, Et al J Clin Pharm. 1994 34, 1077-1082
Hyperkalemia • Plasma potassium over 5.5 mEq/L • Primary problems are weakness and arrhythmias • Bradycardia • Ventricular fibrillation
Increased intake of potassium • Enteral • Parenteral • Transcellular shift of potassium • Lack of insulin • Beta-blockers • Cardiac glycosides • Tissue destruction • Renal potassium excretion • Renal failure • Decreased distal delivery of Na • Hypoaldosteronism Etiologies of hyperkalemia
Hyperkalemia: Clinical Sequelae • Arrhythmia • Paralysis • Due to abnormal nerve conduction • Ascending paralysis mimicking GBS documented with K of 7 • In review of all reported cases of hyperkalemic paralysis: • Ave. K = 9 • Half were on a K sparing diuretic Evers, S. Et al. Secondary hyperkalaemic paralysis. J Neurol Neurosurg Psychiatry 64, 249-252 (1998).
Peaked T waves • Widened QRS complex • The EKG changes into a sinusoidal pattern EKG findings with hyperkalemia • Short QT interval
Treatment of hyperkalemia: Calcium • If EKG signs are present give calcium • Calcium Chloride is more effective than calcium gluconate • Onset of action is instant and duration approx. 1 hour • May repeat until EKG normalizes • Avoid if patient has digoxin toxicity In animal studies, verapamil ablates the cardioprotective effect of calcium. Bisogno, J. L., Langley, A. & Von, D. M. M. Critical Care Medicine. 22, 697-704 (1994). Nugent, M., Tinker, J. H. & Moyer, T. P. Anesthesiology 60, 435-439 (1984).
Stop intake of potassium • Enteral • Parenteral • Induce a transcellular shift of potassium • Insulin • Albuterol • Enhance potassium excretion • Renal • Colonic Treatment of hyperkalemia:
Treatment of hyperkalemia: Speed • N=10, no diabetics • Hemodialysis patients, K = 5.5. • 5 protocols: • Bicarbonate 8.4%. • Bicarbonate 1.4%. • Epinephrine 0.05µg/kg/min • Insulin 5mU/kg/min +Glucose 5mg/kg/min • Hemodialysis w/ 1 K bath Blumberg Et al. Amer J Med; 1988: 85, 507-512.
Bicarbonate for hyperkalemia: duration • N=12 • Hemodialysis patients, K ≥ 5.8. • Given sodium bicarbonate • 4 mmol/min for 1 hour • 0.5 mmol/min for 5 hours • Total 390 mmol • 8 amps of bicarbonate and a liter of fluid for a decrease in K of 0.5 mmol/L At 1 hour the small drop in K was fully accounted for by dilution. At 6 hours 50±7% of the fall in K was due to ECF expansion Blumberg Et al. Kidney International; 1992: 41, 369-374.
Albuterol for hyperkalemia • N=10 • Hemodialysis patients with pre-dialysis K > 5 • Given Nebulized: • Saline. K=5.74 • 10mg albuterol. K=5.93 • 20 mg albuterol. K=5.81 • on separate days. • Patients served as their own controls. Allon Et al. Annals of Int Med; 1989: 110, 426-429.
Albuterol for hyperkalemia: Synergy? • N=12 • Hemodialysis patients with pre-dialysis K > 5 • No diabetics or ß-blockers • Given: • 10 u IV insulin + D50 • 20 mg nebulized albuterol. • Combination of both • Patients served as their own controls. Allon Et al. Kidney International; 1990: 38, 869-872.
Treatment of hyperkalemia: • Move potassium into the cells • Insulin and Glucose • Glucose 0.5-1 Amp • Insulin 10 unit IV • Albuterol • 10-20 mg nebulized • Do not use sodium bicarbonate Cooper, DJ et al, Annals Int Med 1990;112:492-8.
Treatment of hyperkalemia: • Move potassium into the cells • Insulin and Glucose • Glucose 0.5-1 Amp • Insulin 10 unit IV • Albuterol • 10-20 mg nebulized • Do not use sodium bicarbonate Cooper, DJ et al, Annals Int Med 1990;112:492-8.
Treatment of hyperkalemia: • Increase the excretion of potassium • Furosemide (Lasix) • Only in patients with working kidneys • 20 x sCr IV push • Sodium polystyrene resins (Kayexalate) in patients whose kidneys don’t work • 30 g • Dialysis • Make sure the glucose is normal • Rule out urinary obstruction
Life after death • 70-year-old man who developed cardiac arrest secondary to hyperkalemia (K=8.5) from chronic renal failure from obstructive uropathy. • The patient experienced electromechanical dissociation and approximately 26 minutes of asystole after which the resuscitation was suspended • 8 to 10 minutes after declaration of death, as the emergency department personnel were preparing to transport him to the morgue, the patient was noted to have spontaneous respiration. • The patient survived and was discharged without apparent neurologic sequelae. Quick, G Et al. Annals of Emergency Med; 1994: 24, 305-311.