Potassium
Potassium. Major electrolyte in intracellular fluid Normal serum K+ is 3.5 to 5.0 mEq/L Influences both skeletal and cardiac muscle activity 2% is in the ECF is important for neuromuscular function. Potassium. Minor variations are significant Imbalances

Potassium
E N D
Presentation Transcript
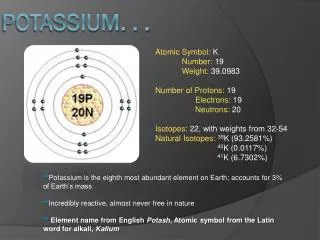
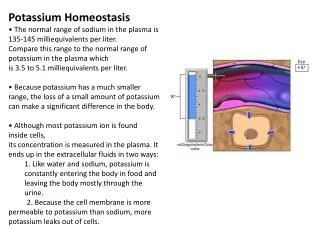
Potassium • Major electrolyte in intracellular fluid • Normal serum K+ is 3.5 to 5.0 mEq/L • Influences both skeletal and cardiac muscle activity • 2% is in the ECF is important for neuromuscular function.
Potassium • Minor variations are significant • Imbalances • Renal system is important in keeping balanced potassium • Body does not conserve potassium • There are no stores. We either have it or we don’t • Gains K thru foods and meds. Elevated K usually doesn’t occur unless there is a reduction in renal function. Renal failure is the #1 cause of Hyperkalemia. K needs to be adjusted daily and your best sources are bananas, apricots, oranges, meats, veggies, potatoes, carrots, dried fruit
Hypokalemia • K+ < 3.5 mEq/L • Cause • GI suction, vomiting, diarrhea • TPN or IVF without K+ replacement • Trauma • Diabetes – if it’s uncontrolled • Low oral intake of K+ • Sweat loss • Medications – diuretics, laxatives, insulin
Renal Loss of K+ • Diuretics • Make you pee more, chances are you’ll pee out some K along with the extra pee • Hyperaldosteronism • High dose Na+ PCNs • Large dose corticosteroids • Greatest risk is in the elderly for developing this. Think about all the old bastards you had to give K-lyte to in clinicals…
S/S Hypokalemia • Fatigue • Anorexia, N/V, Decrease bowel motility • Muscle weakness & leg cramps • Impaired glucose tolerance • Paresthesias (numbness & tingling in the extremities) • Impaired renal concentrating ability • Diminished deep tendon reflexes • Flaccid paralysis – late sign! You’re usually fucked by this time…
S/S Hypokalemia • Increased sensitivity to digitalis • Dysrhythmias • Severe hypokalemia • Hypokalemia commonly accompanies alkalosis.
Memory Jogger for Hypokalemia • SUCTION • S = Skeletal muscle weakness • U = U wave (on the EKG) • C = Constipation • T = Toxicity of Digoxin • I = Irregular or weak pulse • O = Orthostatic Hypotension • N = Numbness or parasthesia
Hypokalemia & Cardiac Changes • strength of contraction • Myocardium irritability • ST segment depression • K+< 2.7 mEq/L may result in PACs, PVC's, V-fib or cardiac arrest • PAC = premature atrial contractions • PVC = premature ventricular contractions • K+< 3.5 assoc. with metabolic alkalosis, high pH & high HCO3 • Digoxin toxicity • B/c hypokalemia potentiates the actions of digoxin
Hypokalemia: Lab Results • K+ deficit < 3.5 mEq/L • K+< 3.5mEq/L often assoc. with metabolic alkalosis, high pH, & high HCO3 • K+< 2.7 may result in dangerous dysrhythmias • pH & HCO3 • Danger signs of low K are dyshrythmias, Cardiac arrest, digoxin toxicity, muscle paralysis (can lead to respiratory arrest)
Medical Treatment Hypokalemia • K+ replacement (PO or IV) • Increase on a daily basis • 40-80 mEq/day • At risk patient • 50-100 mEq/day • K+ rich foods • Green, leafy vegetable and what not • Treat the underlying cause • Is the patient’s magnesium low? Cause if it is, it makes it harder for the kidneys to conserve K
Oral K+ Supplements • Minimize GI irritation • Dilute liquid & effervescent supplement • Give tabs & capsules w/ 8 oz. H2O • Give K+ with food • Adverse reaction – N/V, diarrhea, GI bleed (sometimes)
Oral Potassium Supplements • Avoid overdose (hyperkalemia) • K+ dose if using K+salt substitute • Not used with K+ sparing diuretics • K in the IV is VERY irritating to the vein! Can cause phlebitis very easily.
Intravenous K+ Supplement • Must be diluted! You will DIE!!! • Do NOT give by direct IVP • Max. dose is 60 mEq at a time • Must use IV pump. No gravity allowed! Must be on pump 100% of the time! • Monitor renal output • CHS policy – pt on heart monitor (cause K effects the heart… May not be on monitor if it’s a very low dose) • Monitor IV site (necrosis! Go slowly!) • Neut will neutrilize the K a little bit so the K doesn’t sting as much in their veins when they’re getting it IV
Nursing Interventions: Hypokalemia • Identify pt at risk – esp. if on Digoxin • Monitor EKG (or ECG) & BP • Monitor serum K+ • Pt education – diuretics & laxatives • Administer K+ supplements PO or IV • dietary K+ • Monitor urine output
Hyperkalemia • Serum K+ > 5.5 mEq/L • Causes • Renal failure • Release of K+ from damaged cells • Acidosis • Addison’s Disease • K+ sparing diuretics • High K+ intake • Medications
S/S Hyperkalemia • Main effects cardiac function • Muscle weakness and paralysis • Ventricular conduction is slowed • Paresthesias & irritability • Respiratory and speech muscles • Flaccid muscular paralysis • Legstrunkarms (including respiratory) • GI hyperactivity • N/V, colic, & diarrhea
Hyperkalemia & Cardiac Changes • Slows heart rate • ECG changes • Tall, peaked T wave, short QT interval • Longer PR interval, widening QRS complex • Risk for Heart Block, A-fib, or, V-fib • All of these are severe and we need to fix them as soon as we can, that is, if we can. • The higher the K is the worse these are. Usually associated with a K higher than 7 • Severe K+ • Decreased heart contraction strength • Dilated & flaccid heart
Hyperkalemia: Lab Data • Serum potassium > 5.5 mEq/L • ECG abnormalities • Arterial blood gases – low pH indicating acidosis • Metabolic acidosis is usually accompanied by hyperkalemia
Hyperkalemia Medical Treatment • K+ restricted diet • Stop K containing medications • Monitor for “Digitalis toxicity” • Cation-exchange resins • Kayexalate – PO or PR (in the rectum) • Fastest way to lower your potassium. It’s gross. • 1Gm of resin removes 1 mEq K+ • Dialysis • If conservative methods not suffice
Emergency Medical Treatment Hyperkalemia • Ca Gluconate – IV • Does NOT K+ • Antagonizes K+ action on heart (keeps it from letting the heart get flaccid. Works against the K but doesn’t lower the K levels! This is a quick thing to give them to prevent heart problems) • Monitor ECG • Hypertonic Glucose & Insulin • Insulin - facilitates K+ movement into cells • If you can get things out of the circulating volume and into the cells, it doesn’t have an effect on the body. Unusable when it’s in the cells • Glucose - insulin release from pancreas • NaHCO3 • K+shifts into cells • May be the best thing to move K into the cells quickly! On the test make sure to read the question and look for distracters and pick the appropriate answer
Nursing Interventions Hyperkalemia • Be aware of pt at risk • Monitor for: • Generalized weakness & dysrythmias • Irritability & GI symptoms • Nausea & intestinal colic • ECG or lab abnormalities • Prevention of hyperkalemia • Educate pt: medication & diet • Do NOT draw blood above K+ infusion site • Would have a very high rate of K if you do this. If they have hyperkalemia make sure you know foods that are high in K. I missed the foods he was saying.
Calcium • Serum Ca++ level 8.6 – 10.2 mg/dl (total) • 99% stored in bones (bones & teeth) • Found in three forms: • bound: to proteins (less than 50%) • ionized: found in serum (50% of calcium and is most important) • Children have high levels of this for bone growth • Old people have very low levels of this due to bone loss. • It’s important in muscle contraction, conduction of nerve impulses, cardiac contractility, and helps in the formation of prothrombin • complexed: combined with nonprotein anions: phosphate, citrate, and carbonate
Calcium and Phosphorus • Ca and phosphorus have a reciprocal relationship • If the Ca is low, the phosphorus is high • If the phosphorus is low, the Ca will be high
Ionized Calcium • Activate body chemical rxn • Muscle contractions and relaxation • Promote transmission of nerve impulse • Cardiac contractility & automaticity • Formation of prothrombin
Calcium Regulators • Parathyroid Hormone (PTH) pulls • Releases Ca from the bone • Increases Ca absorption from GI • Increases Ca absorption from renal tubules • When serum Ionized Ca is low, the parathyroid gland releases PTH. Pulls Ca from the bone and promotes movement of Ca (with phosphorus) into the plasma
Calcium Regulators • Calcitonin – secreted by thyroid (keeps) • Antagonist of PTH • Secretion stimulated by high serum Ca++ • Inhibits Ca reabsorption from bone • When Ca levels are too high, the body releases calcitonin which keeps the Ca in the bone which causes a decrease in the Ca levels in your blood
Calcium Regulators • Phosphate • Reciprocal relationship with Ca • Ca = Phos • Vitamin D • Necessary for absorption & utilization of Ca • We get Vitamin D from the sunshine
Hypocalcemia • Serum Ca++ < 8.5 mg/dl • Causes include: - hypoparathyroidism & surgical hypoparathyroidism - malabsorption syndrome - vitamin D deficiency - prolonged admin. of Ca free IVF - acute pancreatitis (Affects PTH secretion, so you’re not able to absorb your Ca) Ca absorption occurs primarily in the Small intestine. If you have Celiacs Disease or something like that, where you can’t absorb stuff, you’ll have low levels of Ca. Lack of Vit D decreases the absorption of Ca
Causes Hypocalcemia • Excessive admin. of citrated blood • Alkalosis • Hyperphosphatemia • Hypomagnesemia • Thyroid cancer • Causes excessive calcitonin secretion • Low serum albumin • Cimetidine (Tagamet) • Interferes with the PTH function • Alcohol Abuse • Medications
S/S Hypocalcemia • Tetany (# 1 sign) • Condition characterized by cramps, convulsions, twitching of the muscles, and sharp flexion of the wrists and ankle joints. Think of tetanus. Tetanus is “Lock Jaw.” Your muscles get stiff and spastic. • Vary with severity, duration & rate of development • Numbness & tingling • Spasms of muscles of extremities & face • Pain
S/S Hypocalcemia • Hyperactive deep tendon reflexes • Abdominal muscle spasms • Respiratory effects • Altered mood & memory • Convulsion/Seizures • Seizures may occur b/c the hypocalemia increases the irritability of the Central Nervous System
S/S Hypocalcemia • Laryngeal spasm • + Trousseau’s • + Chvostek’s • Remember these bitches
+ Trousseau’s Sign • Carpopedal spasm of hand when • Blood supply • Pressure on nerve • Occurs several minutes after BP cuff inflated > systolic BP • Ischemia Indicates tetany and a good sign of hypocalcemia and hypomagnesium
+ Chvostek’s Sign • Spasm of muscles innervated by facial nerve • Tap facial nerve anterior to ear lobe below zygomatic process • They close their eyes and their muscles kind of twitch
Hypocalcemia Cardiac Effects • Prolonged QT interval • Prolonged ST segment • cardiac contractility • sensitivity to Digoxin
Hypocalcemia: Lab Data • Serum calcium levels < 8.5 mg/dl • Albumin/protein levels can give incorrect levels of Ca • Ionized (serum) levels of Ca should be obtained for accurate results (more important physiologically) • PTH levels can effect Ca • Magnesium and phosphorus levels should also be obtained • Remember: • A low Magnesium is equal to a low Ca • A high phosphorus is equal to a low Ca • A high pH is equal to a low Ca
Hypocalcemia Medical Treatment • Acute symptomatic Ca is emergency. • Requires prompt adm. of IV Calcium • 10% Ca-Gluconate • For severe symptoms • Has to be given IV and slowly! Never give IM! • Ca-Chloride • Never give IM • Oral Ca or Vitamin D
Nursing Interventions Hypocalcemia • Identify pt at risk • Hx, labs, etc… • Seizure precautions if severe Ca levels • Monitor airway • Monitor ECG • Educate pt: Ca loss & risks & Ca rich foods • Ca rich foods are milk products, green leafy veggies, canned salmon, sardines, and fresh oysters
Hypercalcemia • Calcium > 10.5 mg/dl • If severe – dangerous with mortality • Causes include: • Hyperparathyroidism (most common cause of hypercalcemia!) • Causes increased bone release of Ca and increased absorption of Ca from the intestines and kidneys • malignant neoplastic disease and chemotherapies • 2nd major cause of Hypercalcemia • thiazide diuretics • prolonged immobilization • Causes and increase in loss of Ca from the bone, moves it into the circulatory system • large doses Vit. D & Vit. A
S/S Hypercalcemia • Decreased neuromuscular excitability: Muscle weakness and incoordination • GI motility: anorexia, N/V, constipation
S/S Hypercalcemia • Altered memory, confusion, slurred speech, lethargy, acute psychotic behavior, & coma • Depressed deep tendon reflexes
S/S Hypercalcemia • Bone pain & abdominal pain • Hypercalcemic crisis: severe polyuria & polydipsia, intractable nausea (you have this all the time and it won’t go away), abdominal cramps, lethargy, coma and cardiac arrest • Can cause kidney stones • Increased urinary calcium concentrations decreases the kidneys ability to concentrate urine. This leads to polyuria and volume depletion
Hypercalcemia Cardiac Changes • Calcium: inotropic effect on heart & reduces heart rate • Effects the contractility of the heart, it’s ability to squeeze down. Because the heart and conduction system are effected by Ca you’ll get dysrhythmias and bradycardia which can lead to cardiac arrest • Shorten ST segment & QT interval • Prolonged PR interval • Potentiate digoxin toxicity
Hypercalcemia: Lab Data • Serum calcium > 10.2 mg/dl • ECG-dysrythmias • PTH- increased (which will throw all the Ca into the blood stream) • X-ray-reveal osteoporosis (cause Ca is being tossed out from the bones into the blood) • Urine (will be high in Ca)
Hypercalcemia Medical Treatment • Treat underlying cause • Dilute serum Ca++ with NS • Lasix/furosemide • IV phosphate • Reciprical thing. Phosphate will pull the Ca down • Calcitonin • Glucocorticoids • Hemodialysis or CAPD • You want to hydrate the pt cause this encourages peeing and excreting the Ca out of your pee
Nursing Interventions Hypercalcemia • Monitor for pt risk • activity & fluids if possible • Ca++ intake • Safety measures for confusion • Monitor ECG, I&O, breath sounds • Monitor for Digoxin toxicity • Prevent Ca++ renal stones • Whenever they get a kidney stone they usually analyze them to see what they’re made of
Magnesium • Normal 1.3 – 2.3 mEq/L • Second most important Ion in the ICF next to K • Mg is important for neuromuscular function • Activator for enzymes • Carbohydrate & protein metabolism • Vasodilation in peripheral arteries • Found in bone and tissue • Eliminated by kidneys • The GI and urinary systems are the best regulator systems for Magnesium
Hypomagnesemia • Mg < 1.3 mEq/L • 1/3 Mg is bound to protein, 2/3 remains as free cation • Causes include: • GI loss -Alcoholism: decrease dietary intake, impairs renal conservation, intestinal malabsorption, intermittent diarrhea and vomiting Kidney is the primary route of Mg excretion. Chronic alcoholism is the most common cause due to poor dietary intake of magnesium
Causes Hypomagnesemia • Intestinal malabsorption syndromes • Diarrhea • Diuretics • Prolonged admin. Mg free IVF/TPN • NG Suction • Renal or liver disease • Diabetic ketoacidosis