Red eye
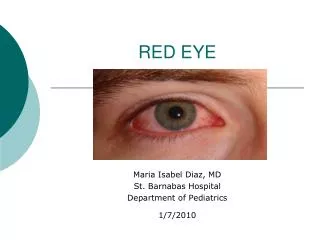
Red eye. Continuity lecture Shanika Uduwana PGY 1. Very common presenting complaint Conjunctivitis (allergic or viral) is probably the most common cause of red eye in the community setting, but a number of more serious conditions can also occur .

Red eye
E N D
Presentation Transcript
Red eye Continuity lecture Shanika Uduwana PGY 1
Very common presenting complaint Conjunctivitis (allergic or viral) is probably the most common cause of red eye in the community setting, but a number of more serious conditions can also occur . Distinguishing patients with red eye who must be referred to an ophthalmologist, from patients who can be managed by the primary care clinician, is important. Measurement of visual acuity and findings on penlight examination are central features in determining management of the red eye. The history and overall patient assessment are useful and confirmatory in the decision to manage or refer.
History Is vision affected? Can the pt still read ordinary print with the affected eye? Patients with impaired vision cannot be managed over the phone; they require a clinician examination and may, depending upon the findings, require ophthalmic referral.
History Is there foreign body sensation? • A foreign body sensation is the cardinal symptom of an active corneal process. • Objective evidence of foreign body sensation, in which the patient is unable to spontaneously open the eye or keep it open, suggests corneal involvement, such patients warrant emergent or urgent referral to an ophthalmologist. • In comparison, many patients report a "scratchy feeling," "grittiness," or a sensation "like sand in my eyes" with allergy, viral conjunctivitis, or dry eyes. This is subjective foreign body sensation and does not necessarily suggest a corneal problem that requires referral.
History Is there photophobia? Is the pt sensitive to bright light? Patients with an active corneal process have objective signs of photophobia as well as objective signs of foreign body sensation.
History Was there trauma? • Did the pt suffer an injury due to a finger poke, a tool, utensil, or other object? Was there blunt trauma such as a fist or tennis ball? Are you a contact lens wearer? • A history of contact lens wear in the setting of discharge and a red eye should increase the suspicion of keratitis
History Is there discharge, other than tears, that continues throughout the day? • Morning crusting followed by a watery discharge for the remainder of the day is characteristic of many self-limited processes • Bacterial conjunctivitis and bacterial keratitis cause opaque discharge that persists throughout the day and requires specific therapy. • Bacterial keratitis, which may or may not affect vision but typically causes objective foreign body sensation and photophobia, requires emergent referral.
Examination • General observation • Measurement of visual acuity • every pt • Both eyes • Penlight examination • Does the pupil react to light? • Is the pupil very small (1 to 2 mm) in size? • Is there purulent discharge? • What is the pattern of redness? (Diffuse/ciliaryflush/hemorrhagic)
Examination • Is there a white spot, opacity or foreign body on the cornea? • Is there hypopyon or hyphema?
Conjunctivitis • The conjunctiva is the mucous membrane that lines the inside surface of the lids and covers the surface of the globe up to the limbus (the junction of the sclera and the cornea). The portion covering the globe is the "bulbar conjunctiva," and the portion lining the lids is the "tarsal conjunctiva.“ • The conjunctiva is comprised of an epithelium and a substantia propria. The epithelium is a non-keratinized squamous epithelium that also contains goblet cells. The substantia propria is highly vascularized and is the site of considerable immunologic activity.
Conjunctivitis Infectious • Bacterial • Viral Noninfectious • Allergic • Non-allergic
Conjunctivitis Bacterial conjunctivitis • commonly caused by Staphylococcus aureus, Streptococcus pneumoniae, Haemophilusinfluenzae, and Moraxella catarrhalis. S. aureus infection is common in adults; the other pathogens are more common in children. • spread by direct contact with the patient and his or her secretions or with contaminated objects and surfaces. It is highly contagious. • typically complain of redness and discharge in one eye • purulent discharge continues throughout the day • More purulent discharge appears within minutes of wiping the lids.
Conjunctivitis Viral conjunctivitis • Typically caused by adenovirus, with many serotypes implicated. • May be part of a viral prodrome • Highly contagious • presents as injection; watery or mucoserous discharge and a burning, sandy, or gritty feeling in one eye. • typically only mucoid discharge if one pulls down the lower lid or looks very closely in the corner of the eye. profuse tearing rather than discharge. The tarsal conjunctiva may have a follicular or "bumpy" appearance. There may be an enlarged and tender preauricular node.
Conjunctivitis Allergic conjunctivitis • Caused by airborne allergens contacting the eye that, with specific IgE, cause local mast cell degranulation and the release of chemical mediators • Presents as bilateral redness, watery discharge, and itching • Itching is the cardinal symptom of allergy, distinguishing it from a viral etiology, which is more typically described as grittiness, burning, or irritation. • Pt often has a Hx of atopy, seasonal allergy or specific allergy.
Conjunctivitis Noninfectious, non-allergic conjunctivitis • Usually the cause is a transient mechanical or chemical insult • Patients with dry eye may report chronic or intermittent redness or discharge and may interpret these symptoms as being related to an infectious cause. • Patients whose eyes are irrigated after a chemical splash may have redness and discharge; this is often related to the mechanical irritation of irrigation rather than superinfection. • A patient with an ocular foreign body that was spontaneously expelled may have redness and discharge for 12 to 24 hours. • All of these causes generally improve spontaneously within 24 hours.
Conjunctivitis Red flags • Reduction of visual acuity • Ciliary flush: A pattern of injection in which the redness is most pronounced in a ring at the limbus (the limbus is the transition zone between the cornea and the sclera) • Photophobia • Severe foreign body sensation that prevents the patient from keeping the eye open • Corneal opacity • Fixed pupil • Severe headache with nausea
Corneal abrasions Corneal abrasion is the term most often applied to any defect in the corneal surface epithelium • Classified as traumatic, foreign body related, contact lens related, or spontaneous. • Traumatic- classic corneal abrasion in which mechanical trauma to the eye results in a defect in the epithelial surface. often caused by fingernails, paws, pieces of paper or cardboard, or by a foreign body that has lodged under the lid. • Foreign body related- defects in the corneal epithelium that are left behind after the removal or spontaneous dislodging of a corneal foreign body. typically caused by pieces of rust, wood, glass, plastic, fiberglass, or vegetable material that have become embedded in the cornea. • Contact lens related- defects in the corneal epithelium, left behind after the removal of an over-worn, improperly fitting, or improperly cleaned contact lens. These eyes have suffered a mechanical insult that is not from external trauma, but rather from a foreign body that is associated with specific pathogens. • Spontaneous defects in the corneal epithelium may occur with no immediate antecedent injury or foreign body. Eyes that have suffered a previous traumatic abrasion or eyes that have an underlying defect in the corneal epithelium are prone to this problem
Corneal abrasions Presentation • Typically complain of excruciating eye pain and an inability to open the eye due to foreign body sensation. Often patients are too uncomfortable to work, drive, or read History First rule out first penetrating trauma, and second an infectious. History may allow distinction between the subtypes of abrasion. history is typically less specific. As an example, an infant who suddenly becomes irritable with symptoms in one eye may have scratched the cornea with a fingernail. Any time a child cannot or will not open an eye, penetrating trauma must be ruled out
Corneal abrasions Examination • Excluding penetrating trauma • Visual acuity • If the exam is difficult in a child, a single drop of topical ophthalmic anesthetic may be instilled to facilitate the remainder of the exam. The child and the caregivers should be warned that the drops will sting. • Penlight and fundoscopic examination • Fluorescein examination
Corneal abrasions Foreign body removal • If a corneal foreign body is detected, attempt to remove it by irrigation. particularly helpful in the case of multiple superficial foreign bodies. Then attempt remove the foreign body with a swab after instillation of topical anesthetic, using direct visualization. • Foreign bodies under the lid should be removed after flipping the lid. If it cannot be dislodged by irrigation or with a swab, the patient should be treated by an individual trained and supervised in the use of instruments to dislodge foreign bodies off the ocular surface. This procedure is performed using magnification (usually a slit lamp, sometimes loupes) and a metal instrument. Topical anesthetic is instilled in the eye. The instrument used can be a 25G needle or a foreign body spud. Appropriate technique, including patient instruction, tangential approach to the cornea, and stabilization of the hand on the zygoma, is required to insure patient cooperation and to avoid further injury to the cornea.
Those without formal training should not approach the globe with sharp instruments; an appropriately trained clinician should be consulted if removal with a swab is unsuccessful. The foreign body should be removed within 24 hours. The patient should be treated in the meantime with a topical antibiotic ointment (eg, erythromycin) four times a day and no patch. After removal of a foreign body containing iron there is often a residual rust ring and reactive infiltrate. Patients with rust ring should be treated as patients with corneal abrasions. The rust ring itself is not harmful and will usually resorb gradually. If there is failure of the epithelium to heal after 2-3 days, debridement of rust ring can be considered by clinicians trained in the use of instruments at the slit lamp. Removal of rust ring on a routine basis at time of foreign body removal is not recommended because of potential damage to Bowman’s membrane and resultant scarring. Corneal abrasion should never be treated with topical steroid.
Corneal abrasions Important • The possibility of penetrating trauma should always be considered when first assessing a patient with an abrasion and ruled out by penlight examination. • Contact lens wearers should never wear a patch for symptom relief. • No patch should be left in place for more than 24 hours. • Any patient with a corneal infiltrate, white spot, or opacity should be seen by an ophthalmologist on the day that finding is noted. • Any patient who has a larger epithelial defect at 24 hours, who has purulent discharge, or who has experienced a drop in vision of more than 1 to 2 lines, should also be seen by an ophthalmologist.
Infectious keratitis Bacterial- • Warrants evaluation by an ophthalmologist on the same day • Bacterial pathogens include Staphylococcus aureus, Pseudomonas aeruginosa, coagulase-negative Staphylococcus, diphtheroids, Streptococcus pneumoniae, and polymicrobial isolates. • Overnight wear of contact lenses is associated with a higher incidence of bacterial keratitis • Breakdown in local or systemic host defense mechanisms, including dry ocular surfaces, topical corticosteroid use, and immunosuppression, can predispose to bacterial keratitis
Infectious keratitis Bacterial – Findings • corneal opacity or infiltrate (typically a round white spot) • It will stain with fluorescein if >0.5mm. • red eye • Photophobia • foreign body sensation • Mucopurulent discharge is typically present • Hypopyon in severe cases Treatment • urgent ophthalmological referral • prompt initiation of topical bactericidal abx • Obtain Cxs before Abx.
Infectious keratitis Viral – • Herpes simplex causes infectious keratitis Findings- • red eye • Photophobia • foreign body sensation • watery discharge. • There may be a faint branching grey opacity on penlight exam. • best visualized with application of fluorescein. Treatment- • Although typically a self-limited process, duration of symptoms is reduced with treatment with topical or oral antiviral agents. • Refer to ophtho
Iritis Inflammation of the anterior uveal tract is called iritis or anterior uveitis • present in a similar fashion to those with an active corneal process • no foreign body sensation • may choose to keep the eyes closed to block out light • will display an aversive response when the penlight is shined in the affected and in the uninvolved eye. • cardinal signs of iritis are ciliary flush and miotic pupil • Typically, there is no discharge and only minimal tearing. Causes- tuberculosis, sarcoidosis, syphilis, toxoplasma, toxocara, and reactive arthritis (formerly called Reiter syndrome) Management- • ophthalmologist within a matter of days • topical steroids, and monitor for side effects and response to therapy
Angle-closure glaucoma Angle closure leads to increased IO pressure Presentation – • appears to be in general distress. • likely to be slumped over covering the eye or clutching the frontal or temporal region of the head with one hand, complaining of headache and malaise. • As intraocular pressure rises, patients develop nausea and in some cases vomiting. • The pain of angle closure is a dull ache that is more likely reported as unilateral headache rather than eye pain. Some patients complain of "the worst headache in my life" and do not attribute their symptoms to the eye • Maybe photophobic • do not typically complain of a foreign body sensation.
Angle-closure glaucoma Penlight examination • red eye • ciliary flush • no discharge. • The pupil is fixed in mid-dilation • anterior chamber is shallow. • Within hours of symptom onset the cornea becomes hazy. Diagnosis is confirmed with measurement of intraocular pressure. Normal intraocular pressure is 8 to 22 mm Hg; pressures in acute angle closure are often greater than 45 mm Hg Treatment- pressure-lowering topical and systemic agents are administered, and definitive treatment in the form of laser iridotomy is performed that same day by the ophthalmologist. The fellow eye is then treated prophylactically within days.
Hyphema • A hyphema appears as a layering of red blood cells in the anterior chamber that may be grossly apparent on visual inspection with a penlight • A grading system based on estimated amount of anterior chamber hemorrhage identifies severity of the hyphema • Complete ocular and orbital evaluation is necessary in a patient with traumatic hyphema because most of these patients will have other eye injuries. • An open globe must be excluded prior to any examination procedure that might apply pressure to the eyeball, such as eyelid retraction or intraocular pressure measurement by tonometry and before any topical agents are applied.
Hyphema • Patients with sickle hemoglobinopathy, bleeding dyscrasia, or suspected open globe need emergent evaluation by an ophthalmologist. In addition, ophthalmology consultation is usually required for all patients to provide comprehensive eye examination, including intraocular pressure measurement. • emergent orbital computed tomography (CT) for patients with a suspected open globe, intraocular foreign body, or serious orbital injury. • Ocular imaging, with CT or ultrasonography, is also recommended for patients with anterior chamber or vitreous hemorrhage that obscures view of the posterior segment. • Hyphema in the presence of trivial trauma may warrant evaluation for systemic disease, eye tumor, clotting disorder, or child abuse.
Hyphema Treatment • Emergency management of patients with traumatic hyphema: • placement of an eye shield, • elevation of the head to 30 degrees, • pharmacologic control of pain and emesis, • treatment of any underlying coagulopathy. • Ophtho referral • Patients should continue to wear an eye shield and restrict activity, including reading, for at least one week or until the hyphema resolves if still present at one week after injury. • surgical clot evacuation in patients with large persistent hyphemas ,early corneal blood staining, or uncontrolled intraocular pressure despite maximal medical therapy (greater than or equal to 50 mmHg for more than five days, or more than 25 mmHg for more than 24 hours in patients with sickle hemoglobinopathy)