Download
1 / 10
130 likes | 898 Vues
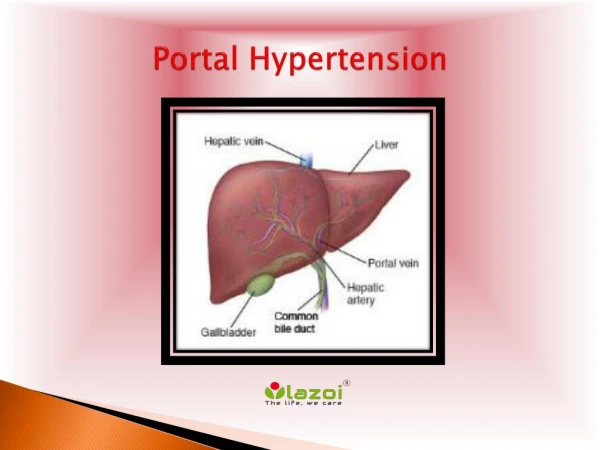
Portal Hypertension. Liver Anatomy. Abdominal Vasculature. Portal Hypertension. Increased resistance to portal blood flow Normal pressure in portal system = 5-8mmHg

E N D
Portal Hypertension • Increased resistance to portal blood flow • Normal pressure in portal system = 5-8mmHg • Increased resistance to portal flow at the level of the sinusoids > due to contraction of vascular smooth muscle and myofibroblasts, disruption of blood flow by scarring and nodule formation • Increase in portal venous blood flow > from hyperdynamic circulation > splanchnic arterial vasodilation > increased flow to portal venous system
Causes Posthepatic • Right heart failure • Constrictive pericarditis • IVC obstruction Prehepatic • Portal vein thrombosis • Splenomegaly • Portal vein narrowing Hepatic • Cirrhosis • Sarcoidosis • Schistosomiasis • Primary biliary cirrhosis • Partial nodular transformation • Budd-Chiari syndrome • Veno-occlusive disease
Consequences • Ascites • Porto-systemic shunts • Splenomegaly • Hepatic encephalopathy
Ascites • Accumulation of excess fluid in the peritoneal cavity • Clinically detectable @ 500mL - MECHANISM • Sodium and water retention > decreased urine output, increased total blood volume • Sinusoidal hypertension > increased hydrostatic pressure • Hypoalbuminaemia > decreased oncotic pressure - COMPLICATIONS • Respiratory distress • Anorexia • Spontaneous bacterial peritonitis • Pleural effusion
Porto-systemic Shunts • Reversal of flow from portal to systemic circulation by dilation of collateral vessels and development of new vessels • Rectum hemorrhoids • Oesophagogasric junction varices • Retroperitoneum • Periumbilical and abdominal wall caput medusae • Oesophageal varices occur in 40%-90% pts with advanced cirrhosis, massive haemorrhage and death in approx half of them. Each bleed ~ 30% mortality
Splenomegaly • Congestive splenomegaly • May cause secondary haematological abnormalities – thrombocytopenia, pancytopenia
Hepatic Encephalopathy • Neuropsychiatric syndrome • acute: drowsy comatose • Chronic: disorder of personality, mood and intellect. Altered sleep patterns. Irritability, confusion, disorientation and slurred speech. Hyperreflexia and increased tone. Coma • Signs: fetor hepaticus, asterixis, constructional apraxia, decreased mental function MECH • Accumulation of toxic metabolites not removed by the liver • Ammonia has a major role – induces alterations of brain neurotransmitter balance • Precipitating factors: Infection, constipation, high dietary protein, GI haemorrhage, fluid and electrolyte disturbances, drugs, surg (TIPS), HCC, cirrhosis