The Arrythmias Chapter 19
The Arrythmias Chapter 19. Pharmacotherapy: A Pathophysiologic Approach The McGraw-Hill Companies. Abbreviations. ACC: American College of Cardiology AF: atrial fibrillation AFFIRM: Atrial Fibrillation Follow-up Investigation of Rhythm Management AHA: American Heart Association

The Arrythmias Chapter 19
E N D
Presentation Transcript
The ArrythmiasChapter 19 Pharmacotherapy: A Pathophysiologic Approach The McGraw-Hill Companies
Abbreviations ACC: American College of Cardiology AF: atrial fibrillation AFFIRM: Atrial Fibrillation Follow-up Investigation of Rhythm Management AHA: American Heart Association ALIVE: Amiodarone versus Lidocaine in Prehospital Ventricular Fibrillation Evaluation ARREST: Amiodarone in Out-of-Hospital Resuscitation of Refractory Sustained Ventricular Tachycardia trial AV: atrioventricular AVID: Antiarrhythmics Versus Implantable Defibrillators trial CASH: Cardiac Arrest Study Hamburg CAST: Cardiac Arrhythmia Suppression Trial CCB: calcium channel blocker CI: contraindicated CPR: cardiopulmonary resuscitation CYP: cytochrome P450
Abbreviations DCC: direct-current cardioversion DM: diabetes mellitus EADs: early after-depolarizations ECG: electrocardiogram ESC: European Society of Cardiology HF: heart failure ICD: implantable cardioverter-defibrillator INR: international normalized ratio IV: intravenous LADs: late after-depolarizations LV: left ventricular LVEF: left ventricular ejection fraction MADIT: Multicenter Automatic Defibrillator Implantation Trial MI: myocardial infarction MUSTT: Multicenter Unsustained Tachycardia Trial
Abbreviations NYHA: New York Heart Association PE: pulmonary embolus PIAF: Pharmacological Intervention in Atrial Fibrillation trial PSVT: paroxysmal supraventricular tachycardia PVCs: premature ventricular complexes RACE: Rate Control versus Electrical Cardioversion for Persistent Atrial Fibrillation RMP: resting membrane potential SA: sinoatrial SCD: sudden cardiac death TIA: transient ischemic attack TdP: torsade de pointes TEE: transesophageal echocardiography VF: ventricular fibrillation VT: ventricular tachycardia WPW: Wolff-Parkinson-White syndrome
Overview • Pathophysiologic mechanisms of arrhythmias • Vaughan-Williams antiarrhythmic classification • Antiarrhythmic drugs • Treatment goals • Treatment • Monitoring • Stroke risk factors in atrial fibrillation • Antithrombotic regimens
Overview • Acute & chronic arrhythmia treatments • Non-drug therapies • Life-threatening proarrhythmias • Risk factors for incessant ventricular tachycardia induced by type Ic antiarrhythmics • Drugs that lead to repolarization & prolonged QT interval cause torsades de pointes • AV block ECG characteristics & predisposing factors
Key Concepts • Use of antiarrhythmic drugs in the US has declined due to major trials showing increased mortality associated with use • recognition of proarrhythmia as significant adverse effect • advancements in nondrug therapy technology • ablation • implantable cardioverter-defibrillator (ICD) • Antiarrhythmic medications frequently cause adverse effects, complex pharmacokinetics
Key Concepts • Amiodarone: most commonly used antiarrhythmic • Patients with atrial fibrillation (AF) • therapeutic goals • control ventricular response • prevent thromboembolic complications • restore/maintain sinus rhythm
Key Concepts • Patients with significant ventricular tachycardia (VT) or ventricular fibrillation (VF) who are successfully resuscitated are high risk for sudden cardiac death (SCD) • should receive ICD • Consider ICD implantation for 1˚ SCD prevention in high-risk patients • history of MI, LV dysfunction, New York Heart Association (NYHA) class II or III heart failure (HF) from either ischemic or nonischemic causes
Key Concepts • Life-threatening ventricular proarrhythmias generally take 2 forms • sinusoidal/incessant monomorphic VT • type Ic antiarrhythmic drugs • Torsades de Pointes (TdP) • type Ia antiarrhythmic drugs • type III antiarrhythmic drugs • many other noncardiac drugs
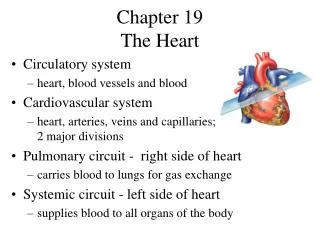
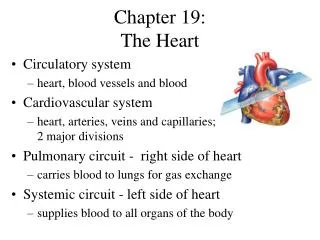
Normal Conduction • Electrical activity initiated at sinoatrial (SA) node • highest rate of spontaneous impulse generation • Moves through cardiac tissue to ventricles at the atrioventricular (AV) node • Flows down bundle of His to bundle branches & the Purkinje system • 2 bundle branches on left; 1 on the right • Impulse reaches refractory tissue (recently excited) & dies out • SA node recovers & fires again
Normal Conduction • Electrical gradient between inside & outside of cardiac cell membranes • baseline gradient: resting membrane potential (RMP) • result of different ion concentrations between inside & outside of cells • active membrane ion pumps maintain gradient • especially Na+/K+ pump • intracellular Na+: 5-15 mEq/L, extracellular Na+: 135-142 mEq/L • intracellular K+: 135-140 mEq/L, extracellular K+: 3-5 mEq/L
Normal Conduction • Electrical stimulation/depolarization results in cell membrane potential changes • Action potential (AP) curve results from ion movement across the cell membrane • Curve divided into phases • Threshold point • junction of phase 4 & 0 • change in Na+ permeability
Normal Conduction • Phase 0: initial, rapid depolarization of atrial & ventricular tissues; increase in cell Na+ permeability; Na+ influx; rapid depolarization overshoots electrical potential, brief period of repolarization • Phase 1: transient active K+ efflux; Ca2+ influx • Phase 2: Ca2+ influx balanced by K+ efflux; plateau • Phase 3: membrane permeable to K+ efflux; repolarization • Phase 4: gradual depolarization; constant Na+ leak to intracellular space balanced by K+ efflux; slope determines automatic cell properties
Normal Conduction • Some cardiac conduction cells do not rely on Na+ influx for initial depolarization • depolarize in response to slow Ca2+ influx • mostly in SA/AV nodes • different from Na+ dependent fibers • slower conduction velocity & recovery of excitability • Drugs modify conduction properties of tissues differently • Ions travel across cell membranes via pores or channels formed in response to differences in electrical potential on either side of the membrane
Normal Conduction • Intrachannel proteins form gates that modulate ion flow • activation gates: open during depolarization • inactivation gates close: stop ion movement • 3 cell cycles states: • resting, activated/open, inactivated/closed • SA/AV tissue activation: slow depolarizing current through Ca2+ channels & gates • Atrial & ventricular tissue activation: rapid depolarizing current through Na+ channels & gates
Abnormal Conduction • Tachyarrhythmia: 2 categories • abnormal impulse generation • “automatic” tachycardia • abnormal impulse conduction • “reentrant” tachycardia
Automatic Tachycardias • Latent pacemaker spontaneous impulse generation • Onset unrelated to initiating event such as a premature beat • Initiating beat usually identical to subsequent beats • Cannot be initiated by programmed cardiac stimulation • Usually preceded by • gradual rate acceleration • termination • gradual rate deceleration
Automatic Tachycardias • ↑ phase 4 slope in tissues other than SA node: heightened automaticity • tissues compete with SA node for cardiac rhythm dominance • rate of spontaneous impulse generation in abnormally automatic tissue exceeds that of the SA node • Causes • digitalis glycosides • catecholamines • conditions: hypoxemia, electrolyte abnormalities, fiber stretch (cardiac dilation)
Triggered Automatic Rhythms • Triggered automaticity: possible mechanism for abnormal impulse generation • transient membrane depolarizations during repolarization but prior to phase 4 • may be related to abnormal Ca2+ or Na+ influx • Precipitated by factors that block K+ channels; responsible for repolarization • hypokalemia • Type Ia antiarrhythmic drugs
Reentrant Tachycardias • Normal conduction: impulses from SA node “meet” recently excited tissue in a refractory period • Reentry: indefinite impulse propagation & activation of previously refractory tissue • Premature beat usually initiates reentry: enters both conduction pathways • encounters refractory tissue in one area of unidirectional block, impulse dies out • Proceeds through other pathway with shorter refractory time
Reentrant Tachycardias • Impulse goes through loop of tissue & “reenters” area of unidirectional block backwards (retrograde) • Forward direction pathway (anterograde) has slow conduction characteristics • refractory period has time to recover excitability • Impulse can proceed through tissue & continue around the loop in a circular fashion • Reentrant focus may excite surrounding tissue at a rate greater than that of the SA node • tachycardia results
Functional Reentry Model • Different model of reentry: functional reentrant loop or leading circle model may also occur • Length of the circuit may vary; the area in the middle of the loop is kept refractory by inwardly moving impulse • Creates a small circle, with “head” of the impulse chasing its “tail” • the wave front continuously excites tissue just as it recovers • Theoretical models require a balance of refractoriness & conduction velocity within the circuit
Figure A: Possible mechanism of proarrhythmia in the anatomic model of reentry 1a) Nonviable reentrant loop, bidirectional block (shaded area). 1b) A drug slows conduction velocity without significantly prolonging the refractory period. Impulse is able to reenter the area of unidirectional block (shaded area); slowed conduction through the contralateral limb allows recovery of the block; a new reentrant tachycardia may result. 2a) Nonviable reentrant loop due to lack of unidirectional block. 2b) Instance where a drug prolongs the refractory period without significantly slowing conduction velocity. The impulse moving antegrade meets refractory tissue (shaded area) allowing for unidirectional block. A new reentrant tachycardia may result. DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th Edition: http://www.accesspharmacy.com
Figure A: Possible mechanism of proarrhythmia in the anatomic model of reentry
Figure B: Mechanism of reentry & proarrhythmia • Functionally determined (leading circle) reentrant circuit. Contrast this model with anatomic reentry; circuit not fixed (does not necessarily move around an anatomic obstacle); no excitable gap; all tissue continuously refractory • A drug prolongs the refractory period without reducing conduction velocity. Tachycardia may terminate or slow due to longer circuit length. Dashed lines represent original reentrant circuit prior to treatment. • A drug slows conduction velocity without prolonging the refractory period (i.e., type Ic agents); accelerates tachycardia due to shorter circuit length. Dashes represent original reentrant circuit prior to treatment. DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th Edition: http://www.accesspharmacy.com
Figure B: Mechanism of reentry & proarrhythmia a) functionally determined (leading circle) reentrant circuit b) a drug prolongs the refractory period c) a drug slows conduction velocity
Reentrant Tachycardias • Does not usually occur in healthy conduction tissue • Heart disease/conduction abnormalities generally present • ischemic/hypoxic damage causes anaerobic glycolysis for ATP production • metabolism causes tissue to slow conduction • changes in discordant manner in different areas of the heart can cause a reentry circuit
Reentrant Tachycardias • Onset usually related to initiating event such as a premature beat • Initiating beat usually different in morphology from subsequent tachycardia beats • Initiation of tachycardia usually possible with programmed cardiac stimulation • Initiation & termination of tachycardia usually abrupt without acceleration or deceleration phase • Examples: atrial fibrillation (AF), atrial flutter, AV nodal or AV reentrant tachycardia, recurrent VT
Antiarrhythmic Drugs • Depression of automatic properties in abnormal pacemaker cells • decreased slope of phase 4 depolarization or elevated threshold potential • if rate of spontaneous impulse generation of the automatic foci < SA node • normal cardiac rhythm can be restored
Antiarrhythmic Drugs • Altered conduction characteristics in reentrant loop pathways • shorter refractoriness in area of unidirectional block • allow antegrade conduction • prolong refractoriness in pathways • prevent retrograde impulse propagation • Antiarrhythmic drugs • alter cardiac conduction in patients + heart disease • Drugs categorized by in vitro electrophysiologic actions
Antiarrhythmic Drugs • Vaughan Williams classification limitations • incomplete, does not include digoxin, adenosine • many agents have properties of more than 1 class • does not incorporate mechanism of tachycardia termination/prevention, clinical indications, side effects • agents “labeled” within a class
Classification of Antiarrhythmic Drugs aVariables for normal tissue models in ventricular tissue. bAlso has type II, β-blocking actions. cClassification controversial. d Not clinically manifest. eVariables for SA & AV nodal tissue only. fAlso has sodium, calcium, β-blocking actions DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th Edition: http://www.accesspharmacy.com
Type I Agents • Block Na+ conduction: “plug up” channels • Channel state affinity • lidocaine, flecainide: block during inactivated state • quinidine: binds when channel is open/activated • Binding & unbinding specific to the receptor • Type Ia: intermediate binding kinetics • Type Ib: fast receptor binding/dissociation • Type Ic: slow receptor binding/dissociation
Type I Agents • Rate dependence (Na+ channel blockade, slowed conduction), greatest at fast HR • slow “on-off” drugs: blockade at normal HR • fast “on-off” drugs: blockade only at rapid HR • Weak bases: pka > 7 • block channel in ionized form • acidosis accentuates actions on Na+ channels • alkalosis diminishes actions on Na+ channels
Type Ia Antiarrhythmics • Quinidine, procainamide, disopyramide • Slow conduction velocity, prolong refractoriness, decrease automatic properties of Na+ dependent conduction tissue • reentry: transform area of unidirectional block into bidirectional block • wave cannot get through pathway in retrograde fashion • area still refractory • Primarily Na+ channel blockers • some effects attributed to K+ channel blockade • used for supraventricular & ventricular arrhythmias
Type Ib Antiarrhythmics • Lidocaine, phenytoin: weak Na+ channel antagonists • Shorten refractoriness without affecting conduction velocity; improve antegrade conduction & eliminate unidirectional block • Lidocaine may work more like Ia agents in diseased tissue • accentuated effects in ischemic tissue caused by local acidosis & K+ shifts that occur in hypoxia • pH changes alter time local anesthetics occupy the Na+ channel, “trap” drug in the cell; increase receptor access • Used primarily in ventricular arrhythmias
Type Ic Antiarrhythmics • Propafenone, flecainide, moricizine • Profoundly slow conduction velocity • Refractoriness relatively unaltered • Eliminate reentry: slow conduction to point where impulse is extinguished & cannot propagate • Potent Na+ blockers • Effective for both ventricular & supraventricular arrhythmias • ventricular arrhythmia use limited by proarrhythmia risk
Type II Agents • β-blockers • Antiarrythmic mechanism: anti-adrenergic actions • SA & AV nodes influenced by adrenergic innervation • Adrenergic stimulation increases conduction velocity, shortens refractoriness & increases automaticity of nodal tissues • β-blockers antagonize these effects • useful for exercise related tachycardias or other tachycardias induced by high sympathetic tone
Type II Agents • Useful in tachycardias where nodal tissues are abnormally automatic or part of a reentrant loop • Interfere with Ca2+ entry into cell by altering catecholamine-dependent channel integrity & gating • β-blockers decrease incidence of SCD after MI • unclear mechanism • Prevent arrhythmias in HF patients • attenuate myocardial remodeling • improve ventricular function
Type III Agents • Bretylium, amiodarone, sotalol, ibutilide, dofetilide • Prolong refractoriness in atrial & ventricular tissue • Delay repolarization: block K+ channels • Inhibit delayed rectifier current (IK) involved in phases 2 & 3 of repolarization • Danger of blocking K+ channel too much: causes arrhythmias such as Torsades de Points (TdP)
Type III Agents • Bretylium depletes catecholamines • increases VF threshold • anti-fibrillatory • no anti-tachycardic effects • ineffective in VT • Amiodarone & sotalol: effective in most supraventicular & ventricular tachycardias • Sotalol inhibits outward K+ movement during repolarization; nonselective β-blocking actions
Type III Agents • Dofetilide (oral only) & ibutilide (IV only) • used for acute conversion of AF or atrial flutter to sinus rhythm • block rapid component of the delayed K+ rectifier current (IKr) • dofetilide can be used to maintain sinus rhythm after conversion
Amiodarone • Characteristics of all Vaughan Williams classes • Na+ channel blocker with fast on/off kinetics • noncompetitive, nonselective β-blocker actions • blocks K+ channels • small degree of Ca2+ antagonist activity • Quick onset with IV administration • Initial action: β-blockade • Predominant effect with chronic use: prolongation of repolarization • Low proarrhythmic potential
Time Course & Electrophysiologic Effects of Amiodarone aRate-dependent. AERP, atrial effective refractory period; AH, atria-His interval; ECG, electrocardiographic effects; EP, electrophysiologic actions; HR, heart rate; HV, His-ventricle interval; VERP, ventricular effective refractory period. DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th Edition: http://www.accesspharmacy.com
Amiodarone • Most commonly prescribed antiarrhythmic • Used in chronic & acute supraventricular/ventricular arrhythmias • Unusual pharmacologic effects, pharmacokinetics, dosing, adverse effects • extremely long t½ (15 to 100 days) • large volume of distribution (Vd) • inhibits P-glycoprotein & most CYP-P450 enzymes • many drug interactions • severe multi-organ toxicities with chronic use
Amiodarone Monitoring DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th Edition: http://www.accesspharmacy.com