Restoring Abdominal Wall Function: The Holy Grail?
640 likes | 1.01k Vues
Restoring Abdominal Wall Function: The Holy Grail?. Brian Jacob MD FACS. Disclosures. Consultant / Teaching/Research Grant: Covidien. Principles for the repair of incisional ventral hernia. Reapproximate the rectus muscles along the midline for ventral hernia repairs to the extent possible

Restoring Abdominal Wall Function: The Holy Grail?
E N D
Presentation Transcript
Restoring Abdominal Wall Function: The Holy Grail? Brian Jacob MD FACS
Disclosures • Consultant / Teaching/Research Grant: Covidien
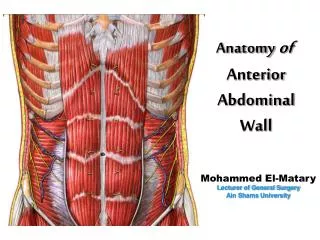
Principles for the repair of incisionalventral hernia • Reapproximate the rectus muscles along the midline for ventral hernia repairs to the extent possible • Attempt to restore the functional, innervated abdominal wall and create a true dynamic repair without undue tension. • The abdominal wall is a load-bearing structure and reacts dynamically to internal and external forces • (hence the need for a ‘‘dynamic repair’’) Incisional ventral hernias: Review of the literature and recommendations regarding the grading and technique of repair The Ventral Hernia Working Group: Karl Breuing, MD, Charles E. Butler, MD Stephen Ferzoco, MD, Michael Franz, MD, Charles S. Hultman, MD, MBA, Joshua F. Kilbridge, Michael Rosen, MD,Ronald P. Silverman, MD, , and Daniel Vargo, MD Surgery: 148, 544-558, 2010
“ ” J Gastrointest Surg. 2010. 14:175
Abdominal Wall Hernia Repair: typical outcome measures • Intraop morbidity • Recurrence rates • Infection rates • Acute and Chronic Pain • Seroma / Hematoma • Ileus and obstruction • Cost
Laparoscopic Ventral Hernia Repair: 9 Year Experience in 850 Patients Heniford BT, Park A, Ramshaw B, Voeller G. Ann Surg, 2003 Complications
Abdominal Wall Hernia Repair: typical patient goals • Reduction of strangulation risk • Resolution of an unsightly bulge • Relief from discomfort / pain • Healing of ulcerated or excess skin • Improvement of abdominal wall function by restoration of abdominal domain?
“Abdominal Wall Function”:what is it and why? • Patient – related endpoint • Coordinated ability, and abdominal wall strength, used to perform all routine activities • Includes breathing, lifting, coughing, bending, working, exercise, etc • Quantify results of the many patient -, technique -, and material – specific variables that can modify hernia outcomes
“Abdominal Wall Function”:why not? • Abdominal Wall Function • Poorly defined • Rarely used • Difficult to assess objectively • Lack assessment tool • May not be relevant
April 2009 SP Bowers
New terms • Functional abdominal wall • Dynamic abdominal wall
Measuring abdominal wall function: not actually such a new concept • Between 1991 and 1999, 235 patients received polypropylene meshes in a sublay position for incisional hernia repair: • 115 patients were implanted with a Marlex heavy-weight mesh (Mhw mesh), • 37 patients with an Atrium heavy-weight mesh (Ahw mesh) and • 83 with a Vypro low-weight mesh (Vlw mesh). • Measured abdominal wall function with 3D stereography • “Data suggested that the use of low-weight large-pore meshes is advantageous for abdominal wall function.” Functional impairment and complaints following incisional hernia repair with different polypropylene meshes. Welty G, Klinge U, Klostemalfen B etal. 2001. Hernia.
What is an adynamic(or poorly functioning) abdominal wall? Using the term “abdominal wall function” as an outcome metric has yet to be accepted
What we don’t want: • Bowel can adhere to polyester surface • Inadequate overlap • Inadequate fixation
Wound Healing: Midline or Defect Closure Mesh / Tissue Interface “The main challenge for surgery is to find the best technique in a given situation (patient, hernia, anatomy), which provides the best overlap…” Uwe Klinge, Aachen, Germany 2011
Matrix deposition: the fibroblast Collagen FIBRILS then bond to form FIBERS
Type I / III Collagen Ratio • Type I: tensile strength (mature collagen) • Type III: thinner diameter, aka immature collagen • Quality of a wound is based on a high type I/III ratio • Reduced ratio (higher proportion of type III) • Reduced stability of connective tissue Junge K, Klinge U, Rosch R etal. (2004) Decreased collagen type I/III ratio in patients with recurring hernia after implantation of alloplastic prosthesis
Type I / III • N = 78; 50 M 28 F • Primary inguinal 25 • Recurrent inguinal 18 • Primary incisional 11 • Recurrent incisional 24 Junge K, Klinge U, Rosch R etal. (2004) Decreased collagen type I/III ratio in patiens with recurring hernia after implantation of alloplastic prosthesis
Type I / III ratio and indication for mesh removal N= 78 explants N=46 N=18 N=14 Junge K, Klinge U, Rosch R etal. (2004) Decreased collagen type I/III ratio in patients with recurring hernia after implantation of alloplastic prosthesis
Type I / III Collagen Ratio • Reduced in patients with recurrent hernias • Provides new possibilities for future research • If I/III could be optimized, perhaps we would create better abdominal wall function Junge K, Klinge U, Rosch R etal. (2004) Decreased collagen type I/III ratio in patients with recurring hernia after implantation of alloplastic prosthesis
N= 24 rabbits • Onlay • Anterior fascia and subcutanous tissue • Sublay (Underlay) • Posterior fascia and rectus • Type I/III ratio assessed • BETTER quality in Sublay position for both mesh materials Hernia. 2010
Poor ingrowth = expensive hernia sac Video clip of shrunken mesh
Collagen Fiber Crosslinking:Wound Strength Increases • Stabilizes the collagen fibers • Resists collagen breakdown by enzymes • Reaches up to 90% strength • Cellular turnover stops Wound Strength 7 14 21 28 35 42 49 56 63 DAYS
Material are not all equal • Ongoing inflammatory processes can last at least a year. • This poor biocompatibility may lead to poor mesh compliance. Ki-67 Novitsky YW, Cristiano JA, Harrell AG, Newcomb W, Norton JH, Kercher KW, Heniford BT. (2008) Immunohistochemical analysis of host reaction to heavyweight-, reduced-weight, and expanded polytetrafluoroethylene (ePTFE)-based meshes after short-and long-term intraabdminal implantations. Surg Endosc. 22: 1070-76
Protein coagulum Platelet adherence Chemoattractant release PMN influx Macrophage, fibroblasts Collagen secretion Connective tissue 80% original strength Why does the material matter? Tissue Ingrowth
Surgeons can use pathophysiology to reduce the risk of recurrences • Mesh implants require sufficient integration within the host tissue to prevent dislocation and reduce recurrences • Bridged mesh does not get incorporated • Wide Overlap in some situations may not be enough Junge K, Klinge U, Rosch R etal. (2004) Decreased collagen type I/III ratio in patients with recurring hernia after implantation of alloplastic prosthesis Kinge U, Prescher A, Klosterhalfen B et al (1997) Development and pathophysiology of abdominal wall defects. Chirurg 293.
Hypothetical defect 10 cm 5cm x 10cm defect [50 cm2]
20 x 15 mesh (5cm overlap) [mesh = 300 cm2]
Closing the defect increases the surface area for tissue ingrowth By adding 50 cm2 of ingrowth, surface area is increased by 20% (50/250)
Current Trends • Evaluating defect size • < 5cm • 5-10cm • >10cm • Using information about the patient to make preoperative AND intraoperative decisions on technique and materials • Not all defects should be treated with a standard laparoscopic IPOM
Outcomes and defect size • Multivariate analysis of 310 consecutive patients with incisional hernias larger than 5cm • Overall recurrence rate was 6% after an average follow-up of 60 months. • A defect size greater than 10 cm is strongly predictive of recurrence after laparoscopic incisional hernia repair • Conclusion: • Defects larger than 10 cm may require a modified laparoscopic technique to increase the mesh / tissue interface Moreno-Egea A, Carrillo-Alcaraz A, Aguayo-Albasini JL. Is the outcome of laparoscopic incisional hernia repair affected by defect size? A prospective study. Am J Surg. 2012;203:87-94