Head Injury
Head Injury. Saurabh Sinha Department of Clinical Neurosciences Western General Hospital. Age Groups. Mechanisms of Injury. What now?. Resuscitation. A airway with cervical spine control B breathing C circulation. Traumatic Brain Injury. Immediate impact injury


Head Injury
E N D
Presentation Transcript
Head Injury Saurabh Sinha Department of Clinical Neurosciences Western General Hospital
Resuscitation • A airway with cervical spine control • B breathing • C circulation
Traumatic Brain Injury Immediate impact injury • Contusions and lacerations • Diffuse damage to white matter • Other types of diffuse brain injury Primary complications • Intracranial haemorrhage • Brain swelling Secondary complications • Brain damage secondary to raised ICP • Hypoxic brain damage • Infection
Aims • Prevent secondary brain injury • Rapid transfer to hospital
Cerebral Physiology • Intracranial pressure (ICP) 0-10 mmHg • Cerebral perfusion pressure (CPP) >60 mmHg • Obligative aerobic glycolysis • Cerebral blood flow (CBF) maitained by autoregulation
Severe Head Injury • Raised ICP • Reduced CPP • Loss of autoregulation • Neuroexcitotoxicity
Raised ICP • Seizures • Brain swelling • Vasogenic oedema • Intracranial haematoma • Hypercarbia • Hypoxia
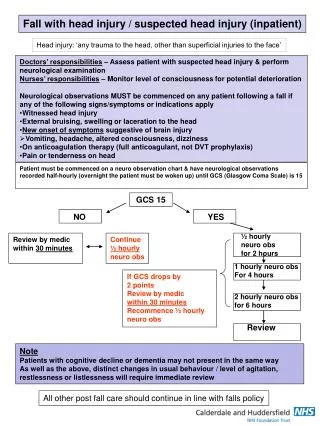
Neurological Assessment • Level of consciousness (GCS) • Pupillary reaction to light • Limb movements • History
Complicating Factors • Alcohol • Drugs • Epilepsy • Stroke • Cervical spine injury
Eye (1-4) open spontaneously open to speech open to pain no opening Motor (1-6) obeys commands localises to pain normal flexion abnormal flexion extension no movement Verbal (1-5) orientated confused inappropriate words incomprehensible sounds none GCS 3-15 Best score using upper limbs Special cases dysphasia periorbital oedema endotracheal tube/tracheostomy The Glasgow Coma Scale and Score
Definition of Coma • GCS 8 or less • No eye opening • Does not speak • Does not obey commands
Signs • Penetrating Injury • Scalp laceration or haematoma • Periorbital haematoma • Blood or CSF from nose • Blood or CSF from ear • Battle’s sign • Cranial Nerve (eye movements, facial weakness)
Indications for skull X-ray • Orientated Patients • History of LOC/amnesia • Suspected penetrating injury (?CT) • CSF/Blood from ear/nose • Scalp laceration (to bone or >5cm), bruise or swelling • Persistent headache or vomiting • Children • Fall from significant height • Onto hard surface • Tense fontanelle • Suspected NAI • Patients with impaired consciousness or neurological signs • All patients unless CT or neurosurgical transfer arranged
Risk of operable intracranial haematoma in head injured patients • GCS 15 (1:3615) 1 in 31300 • With PTA 1 in 6700 • Skull fracture 1 in 81 • Skull fracture & PTA 1 in 29 • GCS 9-14 (1:51) 1 in 180 • Skull fracture 1 in 5 • GCS 3-8 (1:7) 1 in 27 • Skull fracture 1 in 4
Indication for urgent CT/NS referral • Coma persisting after resuscitation • Deteriorating conscious level or progressive neurological signs • Skull fracture & confusion/seizure/neuro symptoms or signs • Open injury: compound depressed #, gunshot or penetrating injury