Head Injury
Head Injury. LAMRT Nov 08. Head injuries. Pathophysiology of brain injury One million patients attend A+E each year in UK with head injury 80% are minor (GCS 13-15) 10% are moderate (GCS 9-12) 10% are severe (GCS <8) Severe head injuries account for 50% of trauma related deaths .


Head Injury
E N D
Presentation Transcript
Head Injury LAMRT Nov 08
Head injuries • Pathophysiology of brain injury • One million patients attend A+E each year in UK with head injury • 80% are minor (GCS 13-15) • 10% are moderate (GCS 9-12) • 10% are severe (GCS <8) • Severe head injuries account for 50% of trauma related deaths
Mechanisms Of Injury Primary brain injuryDamage caused at time of impact Can be focal or diffuse Injury is due to deceleration and shearing forces Dependent on extent of initial injury Difficult to treat Secondary brain injuryInsult imposed after initial injury Due to: Hypoxaemia Hypercapnia Systemic hypotension Intracranial haematoma Intracranial hypertensionEarly treatment is aimed at the prevention of secondary injury
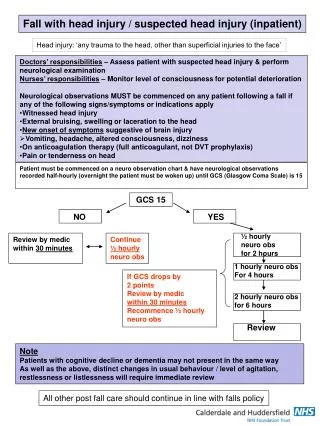
Management • Patients should be managed according to ATLS protocols to prevent secondary brain injury • 5-10% patients with severe head injury have cervical spine injury • Full assessment requires • Glasgow Coma Scale • Pulse, blood pressure • Assessment of pupil diameter and response • Assessment of limb movement • Patients with GCS less than 8 require early intubation
Basal Skull Fracture Signs of basal skull fracture • Blood or CSF from nose or ear • Periorbital haematoma • Mastoid haematoma (Battle's sign)
Extradural haematoma Classic presentation • Transient loss of consciousness with rapid recovery • Lucid interval • Rapid deterioration in level of consciousness • Increased blood pressure. Falling pulse rate • Limb weakness • Pupillary dilatation
Subdural haematoma • Complication of high velocity injury • Patient usually unconscious from the time of injury • Deteriorating level of consciousness