Download
1 / 51
570 likes | 1.44k Vues
Cardiac Conduction Disease Perioperative New Onset Complete Heart Block. Matthew C. Wixson , MD 7 February 2014 University of Michigan Department of Anesthesiology Puerto Vallarta. Objectives . Case presentation Review basic cardiac conduction pathway

E N D
Cardiac Conduction DiseasePerioperative New Onset Complete Heart Block Matthew C. Wixson, MD 7 February 2014 University of Michigan Department of Anesthesiology Puerto Vallarta
Objectives • Case presentation • Review basic cardiac conduction pathway • Review various types of heart block and their implications • Review current guidelines of screening patients with bradyarrhythmias and conduction abnormalities • Educate regarding evidence supporting current practice guidelines • Review basic management of heart block in the urgent/emergent setting
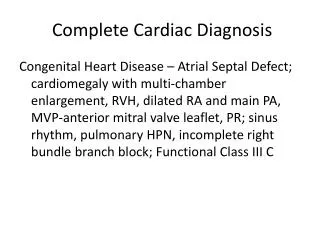
Case Presentation • S.B is a 92 year old ASA 2 male who presents for elective laparoscopic right inguinal hernia repair • PMHx • Mild aortic regurgitation • LBBB • HTN • GERD • Transverse and descending colon CA • PSHx • Inguinal hernia repair • Colon resection • Moh’s resection of SCC
Medications • ASA • Vitamin B12 • Losartan • MVI • Omeprazole • Tamsulosin • Triamterene-HCTZ • Allergies • Lisinopril • Sulfa antibiotics • SHx • Former pipe smoker (45 years, quit 1990) No EtOH or illicit drug use
Studies: EKG– sinus rhythm with occasional PVCs, LBBB • TTE (5/2013): EF ~65%, moderate aortic regurgitation, grade 1 diastolic dysfunction
Clinical Course • Patient presented for surgery on 7/23/2013 • Intraoperative Record: without issues until reversal given (glycopyrrolate 0.4mg, neostigmine 2.5mg) • Patient noted to become bradycardic with HR ~40 beats/minute
PACU Course • Arrived to PACU; report received that patient had been bradycardic since emergence • Had received 0.2mg glycopyrrolate prior to transfer from OR PACU • Arrival vitals: • HR 41 beats/minute • BP 104/48 mmHg • SpO2 (6L NC) 99% • T 36.4 C
Investigations • EKG • Cardiac labs • Telemetry
Patient noted to remain with HR 30s-40s beats/minute throughout PACU course • Had several 4-8 second sinus pauses noted on telemetry • Patient hemodynamically stable and mentating throughout sinus pauses • Transcutaneous pacing pads placed on patient and LifePak20 attached
Cardiology/EP Consult • Initial evaluation: patient noted to be in complete heart block • Requested access for transvenous pacing (if needed) • Patient admitted to SICU for further hemodynamic monitoring • 6 Fr catheter placed into IJ • Arterial line placed • Asymptomatic overnight
Follow-up • Uneventful atriobiventricular pacemaker placement on POD#1 • Episode of atrial fibrillation while hospitalized • Resolved with amiodarone • Patient seen in Cardiology clinic and doing quite well
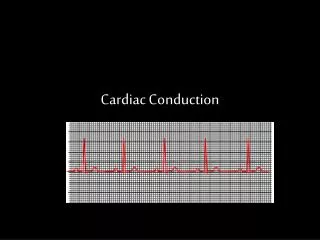
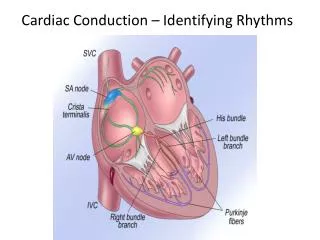
Cardiac Conduction System Review • Major features of EKG • P wave, QRS complex, and T wave • PR interval • PR segment • ST segment • QT interval 1
Cardiac Conduction Image courtesy B. Woodcock
Types of Heart BlockSecond Degree Type II Image courtesy B. Woodcock
Bundle Branch Block • Any conduction block in the His-Purkinje system
Bundle Branch Block • Any conduction block in the His-Purkinje system
Bundle Branch Block • Any conduction block in the His-Purkinje system
Bundle Branch Block • Any conduction block in the His-Purkinje system
Bundle Branch Block • Any conduction block in the His-Purkinje system
Bundle Branch Block • Any conduction block in the His-Purkinje system
Bundle Branch Block Recognition • Right Bundle Branch Block • R and R’ in leads V1 or V2 • Left Bundle Branch Block • R and R’ in leads V5 or V6 • Axis Deviation • Simple rule: thumb test
Screening GuidelinesACC/AHA (2007) “High-grade cardiac conduction abnormalities, such as complete atrioventricular block, if unanticipated, can increase operative risk and may necessitate temporary or permanent transvenous pacing. On the other hand, patients with intra- ventricular conduction delays, even in the presence of a left or right bundle-branch block, and no history of advanced heart block or symptoms rarely progress to complete heart block perioperatively.” 3
Circulation 1978 • 44 patients undergoing 52 operations • 6 temporary pacemakers (TV) placed due to PR prolongation on preoperative EKG • 1 episode of transient CHB observed • 2/6 with TV pacemaker had ventricular irritability 4
Retrospective study of patients with • Prolonged PR interval >0.2s PLUS • RBBB and LAHB (left anterior hemiblock) OR LBBB • 76 patients underwent general, local, or spinal anesthetic • Group 1 (RBBB and LAHB) • 1 patient with sinus bradycardia responsive to atropine • Group 2 (LBBB) • 3 patients with sinus bradycardia responsive to atropine • 3 patients with prophylactic TV pacemaker inserted pre-operatively, none of which were utilized • Conclusion: risk>benefit of placing TV pacer 5
Prospective study at University of Ulm, Germany • Aim: to determine whether presence of 1st degree AV block increases risk of progression to CHB • 103 patients with bifascicular or LBBB • Group 1: 56 patients without AV prolongation • Group 2: 47 patients with AV prolongation • Operations under general or regional anesthesia • Primary endpoint: progression to Mobitz Type II or CHB • Secondary endpoint: asystole >5s or severe bradycardia (<40 bpm) with hemodynamic compromise 6
Results • Group 1 • Two patients progressed to Wenkebach • Three patients had asystole >5 seconds • One progressed to cardiac arrest and was resuscitated • Group 2 • Four patients with HR <40 bpm and hemodynamic compromise • All responsive to atropine • Conclusions: progression is rare • Patients with pre-existing CAD more at risk
Retrospective review of >34,000 cases • 279 patients had complete RBBB • 70/279 had complete RBBB with left or right AD • Results • 1 patient progressed to CHB • On-pump CABG • Conclusion: prophylactic placement of gel pads is not cost-effective 7
Prospective study • Enrollment criteria: asymptomatic bifascicular block OR left bundle branch block • Concurrent 1st degree AV block • Preoperative pacing pads • Increased milliamperes until capture obtained • Scored patient’s pain level 8
Results • 37/39 patients successfully paced • Two patients did not have capture at 120mA • One patient required • 5mg midazolam • 300mcg fentanyl • Assistance with ventilation • Could not increased further due to patient discomfort • 92% reported moderate to intolerable discomfort • No block progression in any patients
Atropine • Anticholinergic (parasympatholytic) • Useful for symptomatic bradycardia • Increases SA nodal rate and automaticity • Increased induction via AV node • Dose 0.5-1.0mg q3-5 minutes • Not helpful in 2nd degree Type II block (Mobitz II) or CHB • Block is normally below AV node in those rhythms 12
Management of Complete Heart Block • Transcutaneous Pacing (TCP) • Non-invasive • Fast • Can initiate while waiting for response to drugs • Useful in hemodynamic instability due to bradycardia • Difference between electrical vs. mechanical capture 12
TCP Diagram Image courtesy B. Woodcock
Transvenous Pacing • More useful for longer-term pacing • Catheter placed in right ventricle • Can place in right atria if atrial pacing necessary • Venous access • IJ • Subclavian • Femoral vein • If prosthetic tricuspid valve, access can be obtained via left side through coronary sinus 13
Complications of TV Catheter Placement • Pneumothorax • Hemothorax • Arterial puncture • Air embolism • Serious bleeding • Myocardial perforation • Cardiac tamponade • Nerve Injury • Thoracic duct injury • Infection • Arrhythmia 13
Indications for Permanent Pacemaker • Class 1 • Generally agreed pacing is indicated • Complete or advanced second degree heart block with symptomatic bradycardia • Persistent complete or advanced second degree heart block following MI • Sinus node dysfunction with symptomatic bradycardia
Class II • Pacemakers frequently used but consensus as to necessity is not clear • Asymptomatic 2º or complete AV block • HR > 40 • Asymptomatic sinus node dysfunction • HR > 40
Class III • Generally agreed pacing is not indicated • First degree AV block • Transient post-MI AV block without bundle branch block • Asymptomatic fascicular blocks without 2nd or 3rd degree AV block
Final Thoughts • Was glycopyrrolate/neostigmine imbalance causative? • Should we have given atropine? • Is it worth placing transcutaneous pads on all patients at risk?
References 1. Sinus Rhythm Labels. www.wikipedia.com/commons 2. Gomella LG, Haist SA. Clinician’s Pocket Reference, Eleventh Edition. 3. ACC/AHA GuidelineACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery. Circulation.2007; 116: e418-e500 4. J O Pastore, P M Yurchak, K M Janis, J D Murphy and L M Zir. The risk of advanced heart block in surgical patients with right bundle branch block and left axis deviation. Circulation. 1978;57:677-680 5. Mikell FL, Weir EK, Chesler E. Perioperative risk of complete heart block in patients withbifascicular block and prolonged PR interval. Thorax 1981; 36: 14-17 6. Gauss A, Hubner C, Radermacher P, Georgieff M, Schutz W. Perioperative risk of complete heart block in patients with bifascicular block and prolonged PR interval. Anesthesiology 1998; 88: 679-87 7. Okamoto A, Inoue S, Tanaka Y, Kawaguchi M, Furuya H. Application of prophylactic gel-pads for transcutaneous pacing in patients with complete right bundle-branch block with axis deviation when surgical procedures are performed: 10-year experience from a single Japanese university hospital. J Anesth (2009) 23:616–619 8. Gauss A, Hubner C, Meierhenrich R, Rohm HJ, Georgieff M, Schutz W. Perioperativetranscutaneous pacemaker in patients with chronic bifascicular block or left bundle branch block and additional first-degree atrioventricular block. ActaAnaesthesiol Scand 1999; 43: 731–736. 9. Maniya R, Aono J, Manabe M. Complete atrioventricular block. Canadian J Anesthesia 1999; 46:3, 265-67 10. Thomson IR, Dalton BC, Lappas DG, Lowenstein E. Right Bundle-Branch Block and Complete Heart Block Caused by the Swan-Ganz Catheter. Anesthesiology 1979; 51: 359-62 • Unnikrishnan D, Idris N, Varshneya N. Complete heart block during central venous catheter placement in a patient with pre-existing left bundle branch block . British Journal of Anaesthesia 91 (5): 747±9 (2003) • Giesecke M, Hosur S. Chapter 55. Cardiopulmonary Resuscitation. In: Butterworth IV JF, Butterworth IV JF, Mackey DC, Wasnick JD, Mackey DC, Wasnick JD, eds. Morgan & Mikhail's Clinical Anesthesiology. 5th ed. New York: McGraw-Hill; 2013. http://www.accessmedicine.com.proxy.lib.umich.edu/content.aspx?aID=57239900. Accessed September 22, 2013. • Hongo RH, Goldschlager N. Chapter 22. Conduction Disorders & Cardiac Pacing. In: Crawford MH, ed. CURRENT Diagnosis & Treatment: Cardiology. 3rd ed. New York: McGraw-Hill; 2009. http://www.accessmedicine.com.proxy.lib.umich.edu/content.aspx?aID=3648856. Accessed September 22, 2013.