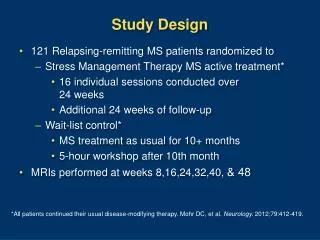
Selecting a Study Design
Selecting a Study Design. Goals. Describe the cohort study design. Describe the case-control study design. Compare situations in which cohort and case-control study designs should be used. About Analytic Studies. We can use analytic studies to test hypotheses. We want to know:

Selecting a Study Design
E N D
Presentation Transcript
Goals • Describe the cohort study design. • Describe the case-control study design. • Compare situations in which cohort and case-control study designs should be used.
About Analytic Studies • We can use analytic studies to test hypotheses. • We want to know: • Whether there is an association between hypothesized exposure and disease, • How strong the association is, • What proportion of cases are due to exposure, and • Whether there is an increased risk of disease with increased exposure (a dose-response relationship). • Two common types of analytic studies are cohort study and case-control study.
What is a Cohort? • A “cohort” is a group of people who have something in common. • Can represent the source population—the population from which cases of disease arise. • Examples of cohorts: • All employees in an office building • Everyone who attended a football game • All the residents of a neighborhood
Cohort Studies • Tend to be retrospective (exposures in the past in relation to disease that has already happened). • Occurrence of disease in exposed group compared to occurrence of disease in unexposed group = risk ratio. • Risk ratio tells whether disease is associated with exposure and strength of association.
Identifying a Cohort • To use a cohort study, you must identify every person in the cohort. • Possible when the group is small and well defined (e.g., wedding reception, cruise ship, school, prison). • Option to interview every member of the cohort or a sample of the cohort.
Identifying a Cohort • Sometimes it may be difficult to define a suitable cohort. • Can you find every single person who ate at the Main Street Deli on January 10-20? • How would you locate every person buying and/or eating contaminated lunch meat from a local supermarket chain? • An alternative: the case-control study.
Case-Control Studies • The most frequently used type of study in outbreaks. • Can be quickly implemented. • Can be used when cohort study might be large and time-consuming. • Identify people with disease (case-patients) and people without disease (controls), then ask everyone about past exposures. • You already know who is sick through doctor diagnosis, lab culture, or health department.
Case-Control Studies • Calculate odds ratio to measure strength of association between illness and exposure. • Compare odds of exposure among case-patients to odds of exposure among controls. • Cannot calculate risk ratio in case-control study.
Selecting Cases and Controls • Defining the source population may help narrow down potential controls. • Do the cases live in the same city or attend the same event? • Are they of a particular race or ethnicity? • Understanding where cases came from will help select your controls. • Controls are a sample of people from the source population.
Selecting Cases and Controls • Example: Outbreak of gastrointestinal illness linked to eating at the Main Street Deli during January 10-20. • Cases recruited from people who ate at the Deli and experienced vomiting. Controls recruited from people who ate at the Deli but did not experience vomiting. • All cases recruited into study; only a portion of healthy controls contacted because could not identify every person who ate at the restaurant during these 10 days. • Want to know what case-patients and controls ate. • Controls selected from customers who ate at the Deli during the time period of interest.
Case-Control or Cohort: Which one is right? • The choice depends on the situation. • Always think about the source population: • Are members of the group easily identifiable? Can you interview all or a sample of them? • Use a cohort study. • Is the cohort difficult to identify or too large to contact all members? • Use a case-control study design.
Retrospective cohort study is the most appropriate study design here. If fewer than 200 people involved, should consider interviewing everyone. Case-Control or Cohort: Which one is right? Figure 1: Easily identifiable cohort (e.g., church picnic, wedding, luncheon) Not ill n=81 Ill n=34 Total N = 115
A case-control study could be used for efficiency here. Or capture entire cohort using e-mail or mail surveys. Or identify cohorts within the larger cohort (e.g., a single dormatory on a college campus). Case-Control or Cohort: Which one is right? Figure 2: Easily identifiable but large cohort (e.g., cruise ship, college campus) Not ill n=2354 Ill n=21 Total N = 2375
Case-Control or Cohort: Which one is right? Figure 3: Selecting controls for a rare disease in a large cohort: case-control design and efficient selection of controls. Hispanic residents in a county Female Hispanic residents in a county Female Hispanic residents of child-bearing age in a county Pregnant Hispanic residents in a county 12 cases of listeriosis among pregnant Hispanic women
Case Studies:Yersinia and chitterlings • 11/15/2001–2/15/2002: 12 cases of Yersinia enterocolitica identified at large urban pediatric emergency department in Tennessee. • Source population: black infants with access to medical care from population served by hospital. • Controls chosen: black infants who presented to the emergency department of same hospital with chief complaint other than gastroenteritis. • Case-control study implicated source of outbreak: • Chitterlings prepared in 100% of case households but only 35% of control households. • Parents able to identify ways kitchen might have become contaminated (e.g., chitterlings cleaned in sink).
Case Studies:Pseudomonas from ear piercing • September 2000: Oregon physician treating 2 patients on 2 consecutive days with infections of the cartilage of the ear; both patients received ear piercings at same kiosk. • Investigators could contact all patrons of kiosk; used a cohort study design: • 118 people received 186 piercings August 1 through September 15. • 7 piercings (4%): laboratory-confirmed Pseudomonas aeruginosa. • 18 piercings (10%): suspected case. • Risk of infection increased if piercing in cartilage rather than earlobe. • The investigators were able to: • Determine the risk of infection among the entire population, • Determine that the risk was different based on site of piercing, and • Identify practices that might have led to contamination of equipment and subsequent infection.
Conclusion • Cohort and case-control studies are both options for determining cause of an outbreak. • Both study the source population. • Cohort uses entire population or representative sample. • Case-control uses all cases of disease and sampled controls. • Both types of studies are effective; your choice will depend on the circumstances of the outbreak you are investigating.
References • Dwyer DM, Strickler H, Goodman RA, Armenian HK. Use of case-control studies in outbreak investigations. Epidemiol Rev. 1994;16(1):109-123. • MacDonald PM, Whitwam RE, Boggs JD, et al. Outbreak of Listeriosis among Mexican Immigrants as a Result of Consumption of Illicitly Produced Mexican-Style Cheese. Clin Infect Dis. 2005; 40:677-682. • Jones TF. From pig to pacifier: chitterling-associated yersiniosis outbreak among black infants. Emerg Infect Dis. 2003;9(8):1007-1009. • Keene WE, Markum AC, Samadpour M. Outbreak of Pseudomonas aeruginosa infections caused by commercial piercing of upper ear cartilage. Jama. 2004;291(8):981-985.