Antibody Identification
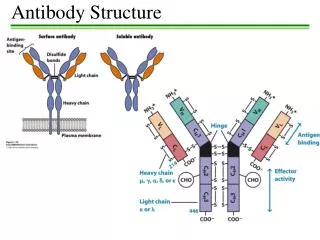
Antibody Identification. Mohammed Jaber. Antibody Presence . Presence of an antibody may be indicated by the following serological tests: A discrepancy in the results of cell and serum ABH grouping. A positive test for unexpected antibodies. A positive direct Coomb’s test.

Antibody Identification
E N D
Presentation Transcript
Antibody Identification Mohammed Jaber
Antibody Presence Presence of an antibody may be indicated by the following serological tests: A discrepancy in the results of cell and serum ABH grouping. A positive test for unexpected antibodies. A positive direct Coomb’s test. An incompatible major cross match.
The Basics….. • As we said in the previous lecture, • Antibody Screens use 2 or 3 Screening Cells to “detect” if antibodies are present in the serum • If antibodies are detected, then they should be identified… present Not present
Why do we need to identify? • Antibody identification is an important component of compatibility testing • It will identify any unexpected antibodies in the patient’s serum • If a person with an antibody is exposed to donor cells with the corresponding antigen, serious side effects can occur (i.e. transfusion reactions).
Key Concepts • In blood banking, we test “knowns” with “unknowns”:- • When detecting/screening and/or identifying antibodies, we test patient serum (unknown that contain blood bank antibodies) with reagent RBCs (known) Known: Unknown: Reagent RBCs + patient serum Reagent antisera + patient RBCs
Reagent RBCs • Screening Red Cells and Panel Red Cells are the same with minor differences: • Screening red cells • Antibody detection/screening • Sets of only 2 or 3 vials • Panel red cells • Antibody identification • At least 10 vials/set
Antibody Panel vs. Screen • An antibody panel is just an extended version of an antibody screen • The screen only uses 2-3 red cells:
Antibody Panel • While antibody panel usually includes at least 10 panel cells: (8-16 group O RBCs)
Panel Red Cells • Group O red blood cells obtained from donors
Panel Red Cells • Each of the panel cells has been antigen typed (shown on antigram) • + refers to the presence of the antigen • 0 refers to the absence of the antigen Example: Panel Cell #10 has 9 antigens present: c, e, f, M, s, Leb, k, Fya, and Jka
Panel Red Cells • An autocontrol (AC) should also be run with ALL panels Autocontrol Patient RBCs + Patient serum
Panel Red Cells • The same phases used in an antibody screen are used in a panel • IS • 37°C • AHG
1 2 3 4 5 6 7 8 9 10 11 Antibody ID Testing • A tube is labeled for each of the panel cells plus one tube for AC: AC 1 drop of each panel cell + 2 drops of the patients serum Do not forget to write patient name and ID, Lab No. Patient cells Patient serum
IS Phase • Perform immediate spin (IS) and grade agglutination; inspect for hemolysis • Record the results in the appropriate space as shown: 2+ 0 0 Up to the Last tube
(LISS) 37°C Phase • 2 drops of LISS are added, mixed and the mixture is incubated for 10-15 minutes • Centrifuge and check for agglutination • Record results as previous but now fill the 37°C lane.
(LISS) 37°C Phase 2+ 0 0 0 0 0 2+ 0 0 2+ 0 2+ 0 0
IAT Phase (or AHG) • Indirect Antiglobulin Test (IAT) – we’re testing whether or not possible antibodies in patient’s serum will react with RBCs in vitro • To do this we use the Anti-Human Globulin reagent (AHG) • Polyspecific AHG • Monospecific Anti-IgG • Monospecific Anti-Complement
IAT (AHG) Phase • Wash red cells 3X with saline (manual or automated (cell washer)) • Add 2 drops of AHG and gently mix • Centrifuge • Read for agglutination • Record reactions
IAT (AHG) Phase 2+ 0 0 0 0 0 0 0 0 2+ 0 0 0 0 0 0 0 0 2+ 0 0 0 0 0 2+ 0 0 0 0 0 0 0 0 0 0 0
And don’t forget…. ….add “check” cells to any negative AHG !
You have agglutination…now what? CC 2+ 0 0 0 0 0 0 0 0 2+ 0 0 0 0 0 0 0 0 2+ 0 0 0 0 0 0 0 2+ 0 0 0 0 0 0 0 0 0 ??
Interpreting Antibody Panels • There are a few basic steps to follow when interpreting panels • “Ruling out” means crossing out antigens that did not react • Circle the antigens that are not crossed out • Consider antibody’s (from the circled) usual reactivity • Look for a matching pattern
Always remember: An antibody will only react with cells that have the corresponding antigen; antibodies will not react with cells that do not have the antigen
1. Ruling Out 2+ 0 0 0 0 0 0 0 0 2+ 0 0 0 0 0 0 0 0 2+ 0 0 0 0 0 2+ 0 0 0 0 0 0 0 0 0 0 0 Cross out antigens that show NO REACTION in any phase; do NOTcross out heterozygous antigens that show dosage.
2. Circle antigens not crossed out 2+ 0 0 0 0 0 0 0 0 2+ 0 0 0 0 0 0 0 0 2+ 0 0 0 0 0 2+ 0 0 0 0 0 0 0 0 0 0 0
3. Consider antibody’s usual reactivity 2+ 0 0 0 0 0 0 0 0 2+ 0 0 0 0 0 0 0 0 2+ 0 0 0 0 0 2+ 0 0 0 0 0 0 0 0 0 0 0 Lea is normally a Cold-Reacting antibody (IgM), so it makes sense that we see the reaction in the IS phase of testing; The E antigen will usually react at warmer temperatures
4. Look for a matching pattern E doesn’t match and it’s a warmer rxn Ab 2+ 0 0 0 0 0 0 0 0 2+ 0 0 0 0 0 0 0 0 2+ 0 0 0 0 0 2+ 0 0 0 0 0 0 0 0 0 0 0 …Yes, there is a matching pattern!
Interpretation: anti-Lea
Guidelines • Again, it’s important to look at: • Autocontrol • Negative - alloantibody • Positive – autoantibody or DTR (i.e. alloantibodies) • Phases • IS – cold (IgM) • 37° - cold (some have higher thermal range) or warm reacting • AHG – warm (IgG)…significant!! • Reaction strength • 1 consistent strength – one antibody • Different strengths – multiple antibodies or dosage
About reaction strengths…… • Strength of reaction may be due to “dosage” • If panel cells are homozygous, a strong reaction may be seen • If panel cells are heterozygous, reaction may be weak or even non-reactive • Panel cells that are heterozygous for an antigen should not be crossed out because antibody may be too weak to react (see previous example)
Guidelines (continued) • Matching the pattern • Single antibodies usually shows a pattern that matches one of the antigens (see previous panel example) • Multiple antibodies are more difficult to match because they often show mixed reaction strengths
Rule of three • The rule of three must be met to confirm the presence of the antibody • A p-value ≤ 0.05 must be observed • This gives a 95% confidence interval • How is it demonstrated? • Patient serum MUST be: • Positive with 3 panel cells with the antigen, +ve reaction. • Negative with 3 cells without the antigen and should not be reacting.
Our previous example fulfills the “rule of three” 2+ 0 0 0 0 0 3 Positive cells 0 0 0 2+ 0 0 0 0 0 0 0 0 2+ 0 0 0 0 0 3 Negative cells 2+ 0 0 0 0 0 0 0 0 0 0 0 Panel Cells 1, 4, and 7 are positive for the antigen and gave a reaction at IS Panel Cells 8, 10, and 11 are negative for the antigen and did not give a reaction at IS
What if the “rule of three” is not fulfilled? • If there are not enough cells in the panel to fulfill the rule, then additional cells from another panel could be used • Most good (I do not know if we are good or not!!) labs carry different lot numbers of panel cells
Patient Antigen Typing (Phenotyping) • In addition to the rule of three, antigen typing the patient red cells can also confirm an antibody • How is this done? • Only perform this if the patient has NOT been recently transfused (donor cells could react (chimera)). • If reagent antisera (of the suspected antibody) is added to the patient RBCs, a negative reaction should result…Why?
Remember Landsteiner’s Rule Individuals DO NOT make allo-antibodies against antigens they have
Multiple antibodies • Multiple antibodies may be more of a challenge than a single antibody • Why? • Reaction strengths can vary • Matching the pattern is difficult
So what we have to do? • Several procedures can be performed to identify multiple antibodies • Selected Cells • Neutralization • Chemical treatment • Proteolytic enzymes • Sulfhydryl reagents • ZZAP
1- Selected Red Cells • Selected cells are chosen from other panel or screening cells to confirm or eliminate the antibody. • The cells are “selected” from other panels because of their characteristics. • The number of selected cells needed depends on how may antibodies are identified.
Selected Red Cells ….. Cont’d • Every cell should be positive only for each of the antibodies and negative for the remaining suspicious antibodies • For example: • Let’s say you ran a panel and identified 3 different antibodies (you cannot rule out): anti-S, anti-Jka, and anti-P1 • Selected cells could help…
Selected Red Cells ….. Cont’d Ag they have Reaction pattern These results show that instead of 3 antibodies, there are actually 2: anti-S and anti-Jka
2- Neutralization • Some antibodies may be neutralized as a way of confirmation • Commercial “substances” bind to the antibodies in the patient serum, causing them to show no reaction when tested with the corresponding antigen (in panel)
Neutralization ….. Cont’d • Manufacturer’s directions should be followed and a positive dilutional control should always be used • The positive dilutional control contains saline and serum (no substance is added) and should remain positive with panel cells. • A control shows that a loss of reactivity is due to the neutralization and not to the dilution of the antibody strength when the substance is added
Neutralization ….. Cont’d • Common substances • P1 substance (derived from hydatid cyst fluid) • Lea and Lebsubstance (soluble antigen found in plasma and saliva) • Isubstance can be found in breast milk **you should be aware that many of these substances neutralize COLD antibodies; Cold antibodies can sometimes mask more clinically significant antibodies (IgG), an important reason to use neutralization techniques
3- Again: Proteolytic Enzymes • Can be used to enhance or destroy certain blood group antigens • Several enzymes exist: • Ficin (figs) • Bromelin (pineapple) • Papain (papaya) • In addition, enzyme procedures may be • One-step • Two-step
Enzymes • Enzymes remove the sialic acid from the RBC membrane, thus “destroying” it and allowing other antigens to be “enhanced” • Antigens destroyed: M, N, S, s, Duffy • Antigens enhanced: Rh, Kidd, Lewis, I, and P