Cellular Receptors
540 likes | 693 Vues
Cellular Receptors. Chapter 2. Binding of Drugs in/to Cells. Receptor = Drug “target” Membrane protein Enzyme Nucleic acid Most drugs bind receptors by weak, noncovalent forces (what are these?) May be reversed by pH change. Molecular Recognition Specificity. Cellular specificity

Cellular Receptors
E N D
Presentation Transcript
Cellular Receptors Chapter 2
Binding of Drugs in/to Cells • Receptor = Drug “target” • Membrane protein • Enzyme • Nucleic acid • Most drugs bind receptors by weak, noncovalent forces (what are these?) • May be reversed by pH change
Molecular Recognition Specificity • Cellular specificity • Not all receptors in all cells, tissues • Receptors selectively bind partic ligands • Stereoselectivity • No drug completely specific
Ligand/Receptor Interactions • Reversible, bimolecular reaction • D + R DR DR* Response • Where R*=Receptor w/ conform’n change • Each will have rate constant • What does this remind you of??
Activating Drugs = Agonists • Drug/receptor binding • conform’l change in receptor • act’n “downstream” cell biochem pathway(s) • tissue response • May bind at separate site on receptor • “Allosteric modulators” • Increases response to natural agonist
Some definitions • Affinity = tendency to bind receptor • Specificity • Association/dissociation constant • Efficacy = tendency to activate receptor • Full agonists elicit max response • Partial agonists elicit submaximal response
Antagonists Bind Receptors… • BUT no activation occurs • No conform’l change in receptor, so no pathway response • May keep agonists from binding • Competitive • Book ex: curare blocks ACh from receptors of neuromuscular junction inhib’n muscle depolarization paralysis • Allosteric modulators may decrease natural agonist binding • Best antagonists have efficacy=0
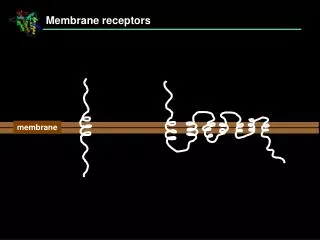
Receptor Superfamilies • Ligand-gated ion channels • G protein-coupled receptors • Receptor tyrosine kinases • Nuclear hormone receptors
Ligand-Gated Ion Channels • Brain, periph NS, excitable tissues (heart), neuromuscular junction • Nicotinic cholinergic receptors (neuromusc) • GABA receptors (brain) • Glutamate receptors (brain) • change membr potential fast synaptic transmission • Complex prot’s w/ multiple subunits
Book Ex: Nicotinic Receptor • Number of subunits differs w/ tissue • Antagonists differ • Allows selective blockade neuromuscular junction • Multiple binding sites for Ach • Excitatory • incr’d Na+/K+ permeability incr’d depol’n incr’d probability of action potential • Direct transduction (no biochem intermediates)
Allosteric modulators may increase/decrease transmitter response in ligand-gated channels • Ex: benzodiazepines • Antianxiety; sleep disorders • Bind GABA ligand-gated receptors • GABA inhibitory • Increases ability of GABA to open channels
G Protein Coupled Receptors • Single subunit • 7 helices span bilayer • Agonists may bind extracell N-terminal domain, or between helices • Few allosteric modulators known • Cytoplasmic loop couples to G protein
G Proteins • Intermediary mol’s • Bind guanine nucleotides • Extrinsic (periph) prot’s at inside bilayer • Anchored to membr by fa chain • Shuttle between receptor, target prot’s • 3 subunits • GTPase activity by a
“Resting state” G prot – trimer w/ GDP occupying site on a subunit • Agonist binding receptor conform’l change w/in cytoplasmic domain • Receptor acquires high affinity for G prot binding G prot to receptor • GTP replaces GDP • bg duplex dissoc’s from a-GTP • Diffuse along membr • Assoc w/ enzymes, ion channels act’n or deact’n
Term’n activity w/ hydrol Pi from GTP w/ GTPase activity of a subunit • Trimer reunites • Single agonist binding can activate sev G-prot mol’s for sev prod’s/act’n results • Amplification
Sev types G prot’s • Interact w/ diff receptors • Control diff effectors • Gs stim’s enz adenylate cyclase, PLC, others • Gi inhibits ad cyclase, PLC, others • Agonist specificity
Cellular Responses • Amplification of signal through second messengers that activate kinases • cAMP • Phosphatidylinositol • Control regulatory enz’s through covalent mod’n • Large, varied cell responses • GPCRs also control • PLA eicosanoid release • Ion channels depol’n, transmitter release, contractility, etc.
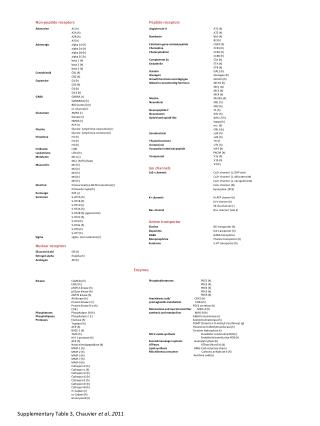
Examples of GPCRs • Receptors for • ACh (muscarinic) • Neuropeptides • Ephinephrine • Muscle (3 types), liver, fat, epithelium, neurons
Receptor Tyrosine Kinases • Single transmembr a helix • Large extracell domain • Agonist binding site • Large intracell domain • Some incorporate tyr kinase activity • Cytokine receptors assoc w/ cytosolic kinases • Agonist binding act’n dimerization • Monomeric form inactive
Dimerized receptors autophosphorylate tyr residues • Phosphorylated tyr attracts, binds SH-2 domain protein • Src Homology • Conserved seq recognizes phosphotyrosine on receptor • Various SH2-domain prot’s allow selectivity for spec receptors • Some are enzymes • Kinases • Phospholipases
Some SH-2 Domain prot’s are couplers for other cell prot’s w/ phosphorylated receptors • Phosphorylation cascades • Impt to cell division, diff’n • Ex: Ras/Raf/MAP kinase pathway • Impt to cancers
SH-2 Domain prot’s as couplers – cont’d • Ex: Jak-Stat Pathway • Impt for cytokines, growth hormone, interferons • Cytosolic kinase phosphorylates receptor dimer • Various Jak’s specificity • SH-2 domain prot’s (Stat’s) attracted, phosph’d, dimerize • Nucleus gene expression
Nuclear Hormone Receptors • Intracellular • Most in nucleus • Some cytoplasmic • Three domains: • Agonist binding domain at C-terminal • Transcriptional control domain • DNA binding domain • Highly conserved • “Zinc fingers”
Ligands lipophilic • Traverse lipid bilayer • Examples: • Steroid hormones • Thyroid hormones • Vitamin D • Retinoic acid • Impt to embryo dev’t
Agonist binding to receptor conform’l change • Dimerization of receptors • Dimers recognize specific base seq’s on DNA near genes • Hormone responsive elements • ~200 bp upstream from genes • Binding DNA may activate or repress gene transcr’n • So “ligand-activated transcr’n factors”
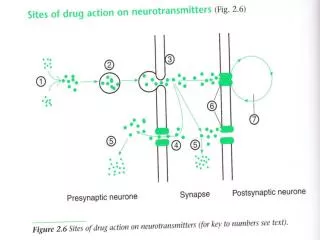
Other Targets of Drugs • Ion Channels • Ligands bind voltage (as well as ligand-gated) channels • Block channel • Affect gating • Activation GPCRs phosph’n channel prot’s • Affect channel opening • Ex: opioids, b-adrenoreceptor agonists • Modulation intracell Ca+2, GTP, ATP • Channels may bind these mol’s • Ex: sulfonylureas act at ATP-gated K+ channels on pancreatic B-cells
Enzymes • Drug may be substrate analog • Competitive or irreversible inhibitor • False substrate • Appears as substrate, so taken up • Not useful as product • Ex: 5-FU blocks DNA synth • Prodrugs • Metabolism active agent
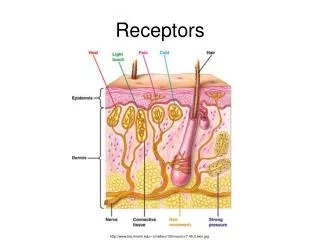
Carrier molecules • Impt for transport across cell membr’s • Have recognition sites for natural mol • Examples: • Cocaine, antidepressants inhibit noradrenaline uptake • Amphetamine acts as false substrate • Loop diuretics affect Na+/K+/Cl- transporter in renal tubule • Cardiac glycosides inhibit Na+/K+ pump
Single Agonist May Have Complex Effects • Families of receptors for agonists • Ex: ACh receptors muscarinic, nicotinic • Further subtypes • Some receptors very specific • Some receptors bind similar ligands • Book ex: dopamine structurally sim to norepi, can stim b1-adrenergic receptors • Multiple receptor subtypes for one ligand can coexist in single cell
Regulation of Receptors • Drugs, agonists decrease sensitivity of receptors to ligands • Fast: desensitization, tachyphylaxis • Gradual: tolerance, refractoriness, drug resistance • Usually w/ continuous exposure • Sensitivity can be increased • Sensitization, desensitization can occur by ligand to same ligand or another
May be due to • Change in receptors • Phosphorylation – inhibits ability to interact w/ G proteins • Slow conform’l change • Exhaustion of mediators • Ex: amphetamines relase amines from nerve terminals; when endogenous amines depleted, drug doesn’t work