Download

1 / 67
670 likes | 849 Vues
in + care Campaign Webinar February 26, 2013. Ground Rules for Webinar Participation. Actively participate and write your questions into the chat area during the presentation(s) Do not put us on hold Mute your line if you are not speaking (press *6, to unmute your line press #6)

E N D
in+care CampaignWebinar February 26, 2013
Ground Rules for Webinar Participation Actively participate and write your questions into the chat area during the presentation(s) Do not put us on hold Mute your line if you are not speaking (press *6, to unmute your line press #6) Slides and other resources are available on our website at incareCampaign.org All webinars are being recorded
Agenda • Welcome & Introductions • Robert Wood Johnson AIDS Program, 15min • Broward County EMA, 15min • Gurabo Community Health Center, 15min • Panel Dialogue and Q&A Session, 15min • Updates & Reminders
Robert Wood Johnson AIDS ProgramNew Brunswick, NJ Roseann Marone, RN
OVERVIEW OF RWJAP – • Located in central NJ—serving patients since 1983- • Evolution of disease in NJ--- went from a very acute to including lengthy hospital admissions to a chronic disease • Receives Part A and D and B funding • Multidisclipinary Team • Member of seven site statewide network
EARLY CONSUMER INVOLVEMENT • Fifteen year process with foundation built from ‘early days’---- • Parents met each other as in patients and at program events
EVOLUTION OF CONSUMER INVOVLEMENT FOR PART D • FAMILY ADVISORY COUNCIL—identified Family Representative • Monthly Executive Committee meetings--Consumer attendees— • Annual Family Day—consumer driven • Annual VOICES Conference-consumer advocacy
PEER MENTOR PROGRAM • Purpose: To encourage women to return to care • Program Coordinator obtains patient permission for PM to contact patient. Release is signed • Patient’s name and phone number shared with PM • PM contacts patient and reviews special needs of patient for returning to care
MAJOR BARRIERS FOR CARE • Personal: family responsibilities, interpersonal relationships, lack of disclosure, lack of acceptance about disease , poor understanding for the need of consistent care, inability to complete paperwork for entitlements, relocation • Medical: treatment fatigue ,untreated or under treated mental illness, relapse, substance abuse • Financial: disconnected phone service, work hours, job loss, under-insured or uninsured , expired ADAP, co-pays for all visits
PEER MENTOR CHECKLIST • Discuss reason for missed appointments, missed refills • Need for blood test • Need for Pap Screening • Need for ancillary specialists--
CHALLENGES • Women are unable to talk during work hours • Concern about disclosing diagnosis • Fear of other family members finding out about their status and need for care
LESSONS LEARNED • Able to reengage women who were not in care • Provided peer to peer support that providers could not do • Shared status promotes greater understanding • Ability to completely understand individual’s situation
Broward County EMA Utilizing Non-Medical Services to Improve Retention in Care Presenters: ShaundelynDegraffenreidt Quality Assurance Coordinator, Ryan White Part A Program Office Ariela Eshel Quality Improvement/Technical Assistance Manager, Broward Regional Health Planning Council
Broward County EMA Snapshot • Over 17,000 People Living with HIV/AIDS in Broward County • Approximately 7,000 Clients Receive Ryan White Part A Program Services Annually • 12 Part A Providers 6 Core Services • Outpatient/Ambulatory Medical Care • Oral Health Care • Pharmaceutical Assistance • Medical Case Management • Mental Health Services • Outpatient Substance Abuse Treatment 4 Support Services • Non-Medical Case Management • Food Bank • Legal Services • Outreach
Clinical Quality Management (CQM) Program • CQM Program Mission • Ensure high quality services are provided to HIV+ Broward residents that meet or exceed HAB’s clinical and other performance measures, through an inclusive structure that integrates consumer and provider input • CQM Program Oversight
In+Care Campaign Involvement • The campaign aims to ensure efforts are aligned with the NHAS to improve access to, and retention in, quality care that will help lower individual and community viral loads • The Broward County EMA elected to participate in the In+CareCampaign in October 2011 • Aligns with the EMA’s vision for delivery of high quality care • Kicked off during an All Networks’ meeting • Network activities are guided by the goal of timely engagement, linkage, retention and coordination of care • Data-Driven, Collaborative Structure • Programmed In+Care retention measures in PE • System-wide aggregate data • Provider specific data • Client-level data
MCM QIP Development • In June 2012, the MCM Network received agency specific client level data for the Gap Measure • 04/01/2011 - 03/31/2012 • Each provider was asked to document the following: • Last Attended Medical Appointment • Reasons for Missed Appointment • Next Scheduled Medical Appointment • Date and Result of Last CD4 Test • Date and Result of Last VL • Data Source for Each Element (e.g., PE, EMR, client self-report)
Gap Measure Definition • Definition: Percentage of patients, regardless of age, with a diagnosis of HIV/AIDS who did not have a medical visit with a provider with prescribing privileges in the last 180 days of the measurement year • Numerator: Number of patients who had no medical visits in the last 180 days of the measurement year • Denominator: Number of patients, regardless of age, with a diagnosis of HIV/AIDS who had at least one medical visit with a provider with prescribing privileges in the first 6 months of the measurement year
Exclusions • Patients documented to be deceased at any time in the measurement year • Patients who were incarcerated for greater than 90 days of the measurement year • Patients who relocated out of the service area or transferred medical care at any time in the measurement year
CD4 and VL Results • Agency A: • 58% detectable, 33% CD4<200 • Agency B: • 21% detectable, 16% CD4<200 • Agency C: • 47% detectable, 20% CD4<200 • Agency D: • 100% detectable, 33% CD4<200 • Agency E: • 90% detectable, 40% CD4<200 • Agency F: • No results submitted
Discussion • Data Entry • EMR indicates client attended appointment • Medical appointment not entered in PE • Client included in the Gap Measure • Case Closure • Incarceration, moving, transferring to another provider, Private Insurance/Medicaid/Medicare • These cases should have been excluded • In some cases, the last documented medical appointment was in May of 2011 with the case remaining open • Progress Note Documentation • Little to no indication that MCMs are tracking medical appointments • In some cases, no communication with client for six months
Questions • How are appointments scheduled and tracked in the MCM Plan of Care to ensure compliance with medical care? • Detectable Viral Load and CD4<200 may indicate non-compliance with care as well as possible eligibility for non-RW funded services (e.g., PAC Waiver). How are MCMs utilizing lab results? • How can MCMs proactively work to prevent clients from falling out of care?
Improvement Plan Accomplishments • Increased provider accountability of client health outcomes • Data driven/collaborative structure • Ability to generate client-level data • Revised client-level outcomes and indicators • Programming of measure per service category • Standing agenda item for all Networks • Peer retention program Challenges • Resolving data integrity issues • Implementing system-wide retention strategies • Barriers and competing needs: • Low income • Housing instability • Lack of transportation • MH/SA related barriers • ADAP crisis and subsequent barriers to accessing medications
Major Accomplishment The EMA received the NQC’s 2012 Award for Performance Measurement The award honors grantees that have significantly strengthened their ability to measure the quality of HIV care and services. The EMA was recognized for its capacity to use an integrated software system to collect data on over 7,000 Part A clients annually, ongoing data-driven QI activities, and refining CQM infrastructure that enhances systemwide performance.
Other Retention Activities • The EMA is the first to pilot the FC/AETC’s Operation HOPEFUL (Healthy Objectives for People Enjoying Full, Uninterrupted Lives with HIV/AIDS) with Medical and MCM providers • A three-year health literacy plan is being implemented • Local Client Level Outcomes and Indicators revised to include retention measures in each service category • Mental Health/Substance Abuse Network QIP Development: • Among the themes identified as impeding retention (severe depression, chronic and persistent mental illness, homelessness, cultural barriers), depression was noted as the greatest indicator of non-retention • The Network is developing trainings for other providers on identifying and addressing mental health barriers to retention
Our Goal • To transition clients along the treatment cascade to full engagement in HIV care and viral load suppression
Next Steps • Routine Data Review and Validation • Monthly QI Data Calls with Providers • Data Findings • Planning Council Process • Implementing QI Projects at System and Provider Levels
Quality Project“In Care Campaign” Preperationby: Denise Vega Alvarado, RN, BSN ClinicalCoordinator Lcda. María Elena López Ramos HealthEducator Marlene Pérez, Program Director
Objectives • Detail the initiatives performed by Program SIVIF under the development of the InCare campaign. • To share methods and strategies established to encourage participant retention • Present analysis and evaluation of the project with the results obtained up to September of the year 2012. • Projections to the year 2013
Background • Program SIVIF providesintergratedservicetoindividualsinfectedwith HIV/AIDS as well as theirfamilies and significantothers. The population of patients in the clinic currently are 278. • Retention campaign was welcomed in our quality program for the initiative to promote retention through the measures established by the National Quality Center. • This considerably is priority for our Center to provide and maintain medical care for our patients. • Under this approach we were able to maximize our efforts in preventing the patient from being out of treatment for a long period of time.
Project Initiation • We initiated with the study and discussion of the four indicators of the retention campaign through a team meeting which forms part of the quality improvement Committee. • Strategies were developed and established to be used in the plan for 2012. • We identified the national measures and the measures established by the AIDS Task Force of San Juan (TGA).
Goal • The overall goal of the campaign's retention in our program is to increase 15% retention of patients receiving services in the SIVIF program and link to treatments according to suggest guidelines for treatments for HIV/AIDS patients health care + by the Department of health and human service (HRSA).
Objectives • Provide services of physicians and link treatment every 3 months. • Provide services of laboratory and in link treatment every 4 months. • Identify absent patients to medical visits and laboratory. • Link newly enrolled patients to treatment within a 30 day period. • Monitoring the viral load of the patient to achieve to reaching levels of less than 200 copies/ml or not detectable.
Determinedgoals • Barriertocare (Gap Measure) Decreaseto= 7% • Frequentvisits(MedicalVisit) Increase: 88% • New patients (PatientsNewly) Increase: 75% • Viral load supression<200 (Load Supresión) Increase: 86%
Work Assignments • Health Educator • Maintains a laboratory registry • Refers lost patients to treatment to Case Manager. • Monitors absences of appointments weekly. • Audit records • Guides and educates the patient about Incare campaign and adherence to treatment. • Clinical Coordinator- • Monitors the compliance of clinical services / processes facilitator / case discussions. • Case Manager- • Search for case and link to treatment (letters, calls, home visits). • Refer to Outreacher patients lost to treatment. • Discussion of cases (medical, nutrition, psychologist). • Educates the participant using the compliance agreement. • Audits of records weekly (last medical visit).
Work Assignments • Nurse- • Identifies absent patient from medical and laboratory appointment. • Register laboratories carried out daily. • Educates participants on the importance of adherence to the treatment and the side effects. • Outreacher- • Case-finding / visits to the home. • Offers free transportation • Coordinates with partner agencies to detox or psychological treatment. • Receptionist- • Identifies the absent patient by using program Proclaim as 'No Show' system. • Confirm appointments and the laboratories the day before their appointment. • Coordinates medical visits every three months and laboratories every four months. • Continuously updates patient demographic information
Work Assignments • Pharmacy- 1. Submits monthly report of patients with poor adherence to treatment. • Medical Personnel • Takes part in the discussion of cases and facilitate strategies for adherence to treatment.
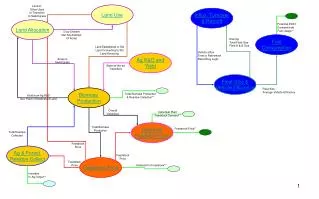
Weekly strategies / Health Educator and Case Management Step # 2 Step # 4 Step # 1 Step # 3
Patient search system Addiction Problems / coordinates with Detox, to link treatment Mental Health Problems /Coordinated service with psychologist in program or with a collaborated agency