Brainstem II
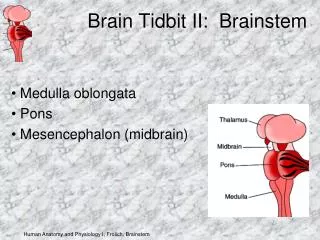
Brainstem II. Tim McDowell October 13, 2010. Objectives. Overview the anatomy and function of CNs VII Facial VIII Vestibulococholar IX Glossopharyngeal X Vagus XI Spinal Accessory XII Hypoglossal nerve Clinical cases and syndromes involving these nerves. Facial Nerve Anatomy.

Brainstem II
E N D
Presentation Transcript
Brainstem II Tim McDowell October 13, 2010
Objectives • Overview the anatomy and function of CNs • VII Facial • VIII Vestibulococholar • IX Glossopharyngeal • X Vagus • XI Spinal Accessory • XII Hypoglossal nerve • Clinical cases and syndromes involving these nerves
Course of Peripheral Nerve: Exits ventrolateral pons (CPA) internal auditory meatus facial canal in petrous bone geniculate ganglion stylomastoid foramenparotid gland
Facial Nerve Function • Motor, parasympathetic, sensory functions • Motor: • Originate in motor facial nucleus (caudal pontine tegmentum) • Brachial motor branches control muscles of facial expression • Temporal, zygomatic, buccal, mandibular, and cervical • Branch off after parotid gland • Innervates stapedius muscle • Branches shortly after geniculate ganglion in mastoid segment
Facial Nerve Function • Sensory: • Taste for anterior 2/3 of tounge • chorda tympanageniculate ganglion • Sensation of portion of external auditory meatus, lateral pinnea and mastoid • greater superfical petrosal nerve geniculate ganglion • Travel as Nervus Intermedius of Wrisberg, receives fibers from geniculate ganglion then travels to rostal nucleus solitarius (taste), and nucleus of the spinal tract of CN V (exteroceptive)
Facial Nerve Function • Parasympathetic • Originate in superior salivatory and lacrmial nucleus (pontine tegmentum) • Travel along nervus intermedius to: • Sphenopalatine ganglion (lacrimal glands, nasal glands) • Submandibular ganglion (sublingual gland, submandibular gland)
Quiz • Which of the following can cause a facial nerve palsy • A Mobius syndrome • B Millard-Gubler Syndrome • C 8 ½ syndrome • D Melkersson-Rosenthal syndrome • E All of the above
Vestibulococholar Nerve • Special sensory function which carries hearing and vestibular sense • Exits brainstem at cerebellopontine angle internal auditory meatus auditroy canal cochlea + vestibular organs
Vestibulococholar Nerve Anatomy: Auditory • Neuroepithelial hair cells stimulated by endolymph causing movement of basilar membrane Cell body spinal ganglion of the cochlear nerve cochlear nuclei (dorsal and ventral) in the lateral medulla • Tonotopic pattern: • Low frequencies (apex of cochlea ventral nuclei) • High frequencies (basal hair cells dorsal nucleus)
Auditory Pathways • Dorsal cochlear nucleus dorsal acoustic striae (decussication) lateral lemniscus inferior colliculus • Ventral cochlear nuclei ventral acoustic striae (trapezoid body)superior olivary nucleus lateral lemniscus IC
Auditory Pathways • Commissural connections between superior olivary complexes, cochlear nuclei, nucleir of lateral lemniscus, and inferior colliculus • Therefore unilateral hearing loss is not seen in CNS lesions proximal to the cochlear nuclei
Auditory Pathways • 3rd order neurons project from inferior colliculus to medial geniculate body (thalamus) • High-freq medial • Low-freq apical-lateral • Auditory radiation white matter tract below putamen temporal lobe (primary auditory cortex- Brodmann’s area 41> audiotry association cortex area 42) • High-freq medial, low-freq lateral
Vestibulococholar Nerve Anatomy: Vestibular • Measures angular and linear acceleration of the headwithin the membranous labyrinth • 3Semicircular canals (angular, measured by cristae inside the ampulla): horizontal, anterior/superior, posterior/inferior • Utricle and saccule (linear, measured by maculae which contain otolith crystals) • Afferent connection to cell bodies of vestibular ganglion of Scarpa (inside internal acoustic meatus) • Superior portion: anterior and horizontal semicircular canals + utricle • Inferior portion posterior semicircular canal + saccule
Vestibular Pathways • Vestibular nerve projects to vestibular nuclei in pontomedullary junction • Superior (of Bechterew) • Lateral (of Deiters) • Medial (of Schwalbe) • Inferior (descending nucleus of Roller) • Semicircular canals superior and medial nuclei • Macular fibers medial and inferior vestibular nuclei • Vestibular nerve also projects inferior cerebellar peduncle vestibulocerebellum (flocculonodualr lobes)
Vestibular Pathways • Output primarily re: feedback integration with cerebellum, spinal cord, and brainstem • Main connectinos: • Medial Longitudinal Fasciculus (conjugate eye mvmts) • Superior vestibular n.ipsilateral • All others contralateral • Medial Vestibulospinal Tract (descending MLF) • Mostly medial vestibular nucleus cervical and upper thorasiccontralateral spinal cord • Lateral Vestibulospinal Tract (facilitates extensor trunk tone + antigravity muscles) • Lateral + inferior vestibular nuclei ipsilateral spinal cord • Cerebellum • Ipsilateral flocculondular lobe + reciprocal connection back thru juxtarestiform body
Weber test: vibration at vertex, localizes to conductive hearing deficit and away from sensorineural hearing deficit • Rinne Test: air/bone cunduction compared in each ear • Dix-Hallpike:
Quiz: • What makes a Dix-Hallpike Positive in BPPV? • Latency • Torsional, upper pole beats towards ground • Fatigability • Rebound • Habituation
Glossopharyngeal Nerve Anatomy • Emerges from posterior lateral sulcus of medulla Jugular foramen widens to superior and petrous ganglia descends on lateral side of pharynx around stylopharyngeus muscle (+innervates) base of tougne
Glossopharyngeal Nerve Function • Motor: • stylopharyngeal muscle • Mildly lower palatal arch • Mild dysphagia • Supplied from nucleus ambiguus • Sensory: • taste +sensation to post. 1/3 of tougne • sensation to soft palate, tonsils, pharyngeal wall, tragus of ear, eustachian tube, mastoid region • Chemoreceptive and baroreceptive afferents from caroitid body + sinus
Glossopharyngeal Nerve Function • Sensory Function continued • For taste + chemo/baro receptors, cell bodies in petrous ganglion, project to solitary nucleus (rostal: taste, caudal: chemo/baro receptors) • Exteroreceptive afferents, cell bodies in both petrous and superior ganglia spinal nucleus of V • Parasympathetic: • Inferior salivatory nucleus otic ganglion (synapse here) (Via V3) parotid gland
Vagus Nerve • Posterior sulcus of lateral medulla, multiple rootlets trunk, exits via jugular foramen • Two vagal ganglia here: jugular (sup) + nodose (inf) • Auricular ramus branches off concha of external ear • Meningeal ramusdura matter of post fossa • Pharyngeal ramus pharyngeal plexus (with IX) • Superior laryngeal nerve (arises near nodose gangion): sensory to larynx + cricothyroid muscle
Vagus Nerve • In neck travels with internal carotid art + IJV) • Cardiac rami: cardiac plexus • Recurrent laryngeal nerves (left longer): all muscles of larynx except cricothyroid • Thorax: give off pulmonary and esphogeal plexus • Abdomen: innervate abdominal viscera
Vagus Nerve • Motor fibers originate from • doral motor nucleus of vagus: preganglionicparasympathetics • nucleus ambiguus: striated muscles • Sensory fibers: • Taste from epiglottis, hard & soft pallates, and pharynx, + general visceral afferents from oropharnyx, larynx, thorax and abdo viscera solitary nucleus (cell bodies in nodose ganglia) • Exteroreceptive sensation from ear spinal nucleus of V (cell bodies in juglar ganglion)
Spinal Accessory Nerve • Pure motor nerve • Cranial root (becomes recurrent laryngeal nerve, mostly travels with X) • Spinal root: dorsolateral portion of ventral horn in cervical spinal cord (rostal portion SCM, caudaltrapezius) • Exit cord between ventral and dorsal nerve rootlets, just dorsal to dentate ligament • Ascend together into skull through foramen magnum exits via jugular foramen neck to supply SCM and trapezius • NB: UMN innervation of SCM is ipsilateral
Hypoglossal Nerve • Motor control of the tougne • Arises from hypoglossal nucleus • Exits medulla as multiple rootlets between pyramid and inferior olivary nucleus hypoglossal foramen • NB UMN fibers cross before innervating hypoglossal nuclei
Quiz: • True or false • Glossopharyngeal neuralgia is commonly associated with MS? FALSE • The most common cause of isolated CN XI is iatrogenic? TRUE
Quiz: • Clinical picture of: • Ipsilateraltrapezius and sternocleidomastoid paresis and atrophy • Dysphonia, dysphagia, depressed gag reflex, and palatal droop on the affected side associated with homolateral vocal cord paralysis, loss of taste on the posterior third of the tongue on the involved side, and anesthesia of the ipsilateral posterior third of the tongue, soft palate, uvula, pharynx, and larynx • Often dull, unilateral aching pain localized behind the ear • Name the lesion. Where is it? Common causes?
Vernet’s Syndrome (Jugular Foramen Syndrome) • Lesion at jugular foramen • Common with glomus jugulare tumors and basal skull fractures
Quiz • Clincial picture of isolated VI and XII paresis: • Godfresdsen syndrome • Clival tumor, often nasopharyngeal, poor prognosis
TABLE 13-1 Syndromes Involving Cranial Nerves IX through XII Other syndromes involving lower CN’s