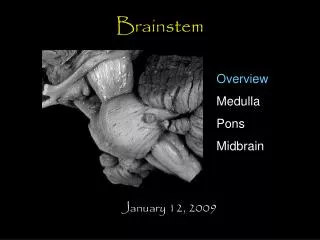
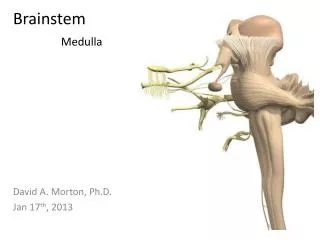
BRAINSTEM
BRAINSTEM . By Joshua Bower Peer Support 2013/2014 J.Bower@warwick.ac.uk. Where do the following CNs emerge from?. CN III+IV V VI-VIII IX+X XI XII. Midbrain Pons Pontomedullary junction Lateral medulla C1-C5 of SC Ventral medulla.

BRAINSTEM
E N D
Presentation Transcript
BRAINSTEM By Joshua Bower Peer Support 2013/2014 J.Bower@warwick.ac.uk
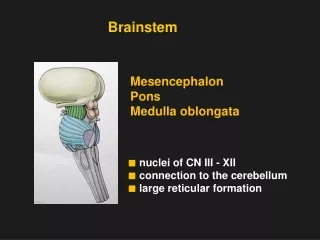
Where do the following CNs emerge from? • CN III+IV • V • VI-VIII • IX+X • XI • XII • Midbrain • Pons • Pontomedullary junction • Lateral medulla • C1-C5 of SC • Ventral medulla
What signs might you expect from an infarction in the black area? [2] • Right ocular palsy • Pupillary changes CN III and IV affected
A patient suffers from a cortical infarction affecting CN VI-VIII. What signs and symptoms will you expect to see? • Limited eye abduction • Diplopia • Bell’s palsy • Loss of balance • Sensorineural hearing loss • Tinnitus
What signs would you expect to see with a UMN lesion of CN VII? • Contralateral facial paralysis, with forehead sparing
Bulbar palsy(i) Is it UMN or LMN?(ii) What nerves are affected?(iii) List FOUR symptoms(iv) List TWO causes • LMN • CN VII-XII • Dysarthria, dysphonia, drooling, poor swallowing, flaccid paralysis, wasting, fasciculations • Due to paralysis of pharynx, soft palate, larynx and tongue • Polio, radiotherapy, CVE
Which nucleus provides motor supply to the pharynx, palate and larynx? • Nucleus solitarius • Nucleus accumbens • Nucleus ambiguus • Nucleus dorsalis • Nucleus pulposus • Nucleus vagus Nucleus ambiguus - gives rise to the branchial efferent motor fibres of CN X
Pseudobulbar palsy(i) Is it UMN or LMN?(ii) What nerves are affected?(iii) List FOUR symptoms(iv) List TWO causes • UMN • Bilateral corticobulbar tracts • Similar to bulbar – but can develop spastic paralysis of pharynx and larynx (airway occlusion emergency) • Head injury, CVE, high brainstem tumour
What system in the brain controls sleep? • Cerebellum • Tuberoinfundibular pathway • Sensory cortex • Posterior parietal lobule • Reticular formation • Periaqueductal gray Reticular formation – complex network of fibres with some defined nuclei (raphe nuclei etc) which controls sleep-waking cycle, pain modulation etc
A severely hypertensive patient with poor compliance with treatment suddenly collapsed and was unconscious. He had pin point pupils, quadriparesis and decerebrate posturing. It was suspected he had suffered pontinehaemorrhage. (i) Explain why a haemorrhage into the pons could cause sudden LOC? Damaged reticular formation
A severely hypertensive patient with poor compliance with treatment suddenly collapsed and was unconscious. He had pin point pupils, quadriparesis and decerebrate posturing. It was suspected he had suffered pontinehaemorrhage. (ii) What else must be damaged in the pons to cause quadriparesis? Descending motor tracts
A severely hypertensive patient with poor compliance with treatment suddenly collapsed and was unconscious. He had pin point pupils, quadriparesis and decerebrate posturing. It was suspected he had suffered pontinehaemorrhage. (iii) The arterial haemorrgage in the pons would escape into his CSF – what effect(s) would this have on CSF appearance and pressure? Blood stained CSF, raised pressure
A severely hypertensive patient with poor compliance with treatment suddenly collapsed and was unconscious. He had pin point pupils, quadriparesis and decerebrate posturing. It was suspected he had suffered pontinehaemorrhage. (iv) Would a lumbar puncture be helpful in this situation? Why/ why not? No – because of the risk of coning with raised ICP
A neurosurgeon evacuated an extradural haematoma. The patient never regained consciousness, was unable to breathe spontaneously and had to stay on a ventilator. Why couldn’t he breathe spontaneously? Brain stem compression – respiratory centre located here
What are the FOUR functions of CN IX?What nuclei do they project from/to? Sensation from pharynx, mid ear etc Spinal nucleus of trigeminal n. Taste from tongue (posterior 1/3) and carotid body and sinus input Nucleus solitarius Motor to stylopharyngeus Nucleus ambiguus Parotid gland secretions Inferior salivatory nucleus
QUESTIONS? By Joshua Bower Easter Revision 2014 J.Bower@warwick.ac.uk