Download

1 / 43
470 likes | 808 Vues
Using Six Sigma in Infection Prevention. Brandi Cavegn MSN, RN – Green Belt. Personal Background. Who am I? And what is my background? Greenbelt- Certified, part time Other Belts? White, Yellow, Green, Black, Master Black. What is Six Sigma. Six Sigma is a problem solving methodology.

E N D
Using Six Sigma in Infection Prevention Brandi Cavegn MSN, RN – Green Belt
Personal Background • Who am I? • And what is my background? • Greenbelt- Certified, part time • Other Belts? White, Yellow, Green, Black, Master Black
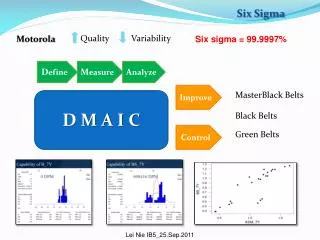
What is Six Sigma • Six Sigma is a problem solving methodology. • Six Sigma minimizes mistakes and maximizes value. • Six Sigma originated in Manufacturing (much like LEAN) but can be used in healthcare successfully. • Six Sigma performance is the statistical term for a process that produces fewer than 3.4 defects (or errors) per million opportunities for defects. (think bell curve). • Six Sigma is often the goal but rarely reached • Six Sigma decreases the “normal variation” in a process.
How Six Sigma tools can be useful to You…. • Variety of tools to be used • Focus is on decreasing variation • Full variety of tools can be used without initiating entire project. • DMAIC Methodology • D- Define • M- Measure • A- Analyze • I- Improve • C- Control
Case Study • NICU CA-BSI project • Use Six Sigma methodology to reduce variation in the insertion and maintenance of Central line catheters in the NICU. • Overall goal was to reduce the infection rate, but this was not the goal of the project. • Disclaimer
D-Business Case (Use Evidence) • An opportunity exists within CHW to reduce the number of blood stream infections associated with catheters in the NICU. It is important to address this issue now because it impacts not only patient safety but key business drivers related to organizational success. • The Agency for Healthcare Research and Quality (AHRQ) and the Centers for Disease Control and Prevention (CDC) have acknowledged that central venous lines are critical components of medical care for many patients, and their use can lead to catheter-associated blood stream infections. • Bloodstream infections account for 30% of all health care associated infections in pediatrics according to the CDC’s National Nosocomial Infection Surveillance System (NNIS). Although the association between bloodstream infections and death is somewhat controversial, AHRQ concluded that findings in the literature are consistent with a 10-20% increase in mortality. • The CDC has reported an average of 2.8 to 12.8 infections per 1000 catheter-days. • Directly aligned to the CHW strategic goal to provide the Best and Safest care • The mean cost of a bloodstream infection has been estimated at $46,133 due to the longer length of stay and additional ancillary utilization (Slonim et al), making it the most expensive of all nosocomial infections. • The financial impact may be greater for CHW because of the NICU population and the possible impact on Neurodevelopment • Line infections can also be categorized as “never events” which are errors in medical care that are clearly identifiable, preventable and serious in their consequences for patients. Never events are not reimbursable under many insurance plans. • Results of the project such as standardized processes or new staff knowledge regarding line insertion, maintenance and infection risks should improve employee satisfaction scores and increase staffs comfort level dealing with catheters • Preventing infection will be a positive driver for patient satisfaction
D- Goal Statement • To reduce bloodstream infections associated with catheters to 1.5 per 1,000 catheter days in the NICU population by year end 2008 • Double the number of days between bloodstream infection occurrences • 100% of patients receive the insertion central line bundle (hand hygiene, maximal barrier precautions (sterile gown, sterile gloves, cap, mask, insertion site toweled off with sterile towels, daily review of line necessity, optimal catheter site selection, chlorhexidine skin antisepsis for patients over 2 months of age) • 95% of patients with a CVL were assessed daily for necessity of retaining the CVL. • 95% of patients receive the line maintenance bundle • Improved communication among staff and standardized work processes regarding the insertion and maintenance of CV lines. • Sigma level 4.47 (1.5 per 1000) Six Sigma would be (.005 per 1000)
D-Project Scope • The scope of the project includes lines placed in the NICU at CHW. • Central Venous Lines (CVL) include: Broviac, Peripherally Inserted Central Catheter (PICC), Umbilical Arterial Catheter (UAC), Umbilical Venous Catheter (UVC) • The team will focus on the process boundaries of line insertion and line maintenance. • The definition of Blood Stream Infections (BSI) as defined by NHSN will be used for data collection purposes. • Catheter Associated –Blood Stream Infection (CA-BSI) Insertion Bundle compliance in the NICU • The project begins in May 2008 and will conclude at the end of December 2008
D-Alignment and Authority • Does this project align with any other business initiatives currently underway? How will we coordinate with the people leading these initiatives? • Infection control • Interventional Radiology • Pharmacy • CAT • Anesthesia • PICU initiatives • What authority do we have to make decisions and implement changes? Include here the authorities we must approach for decisions and approvals beyond our team’s scope. Is there anything that is outside the team’s boundaries? • Product Committee – must evaluate any recommendations on equipment • Infection Control – approval required for any changes to surveillance data • JCPC – review of any new policies • OR – stakeholder involved in patient care process– Rob Omelina is contact person • Purchasing – approval required on recommendation to purchase new supplies • Sterile Processing – approval required on recommendations for cleaning equipment and supplies • Environmental – stakeholder in process and impact patient care environment • Respiratory Care – stakeholder providing care to patient and would need training on any process changes or expectations regarding line insertion and maintenance • Radiology - stakeholder providing care to patient and would need training on any process changes or expectations regarding line insertion and maintenance
M-Preliminary Data on CA-BSI 10 infections in 2007 = 1.65 infections per 1000 line days 8/10 were identified as maintenance related 2/10 were undetermined (3 and 4 days after insertion) 2007 Average days between infections- 36.1 Goal for 2008 is 72.2 (double last year)
A-Opportunity/ Problem Statement • 10 Catheter Related Blood stream Infections were reported in the NICU for 2007 • $46,133 per infection x 10 infections = $461,133 in additional costs • Infections can occur during the line insertion or maintenance period • Insertion Bundle Compliance- evidence based interventions that should be implemented together (hand hygiene, maximal barrier precautions, daily review of line necessity, optimal catheter site selection, chlorhexidine skin antisepsis for patients over 2 months of age) • Maintenance include dressing and tubing changes • 1.65 infections per 1000 line days • Sigma of 4.44
M- Process Maps or Flow charts • A graphic model of the flow of activities, material, and/or information that occurs during a process. • Sets your baseline.
A- Use Your Tools Top-Down: the breaking down of a system to gin insight into its compositional sub-systems Sub-systems:
Line insertions Maintenance Medication Hand washing IP practices
A- SIPOC Tool • Identifies the Voice of the Customer (VOC) • S- Suppliers • Systems, people, organizations, or other sources of the materials, information, or other resources that are consumed or transformed in the process • I- Inputs • Materials, information, and other resources provided by the suppliers that are consumed or transformed in the process • P- Process • The set of actions and activities that transform the inputs into outputs • O-Outputs • The products or services produced by the process and used by the customer • C- Customer • Persons, groups of people, companies, systems, and downstream processes that receive the output of the process
A- FMEA • Failure Mode Effects Analysis • A procedure used to identify, assess, and mitigate risks associated with potential failure modes in a product, system, or process
A-Staff Survey 1) A Clave (Blue end cap) needs to be primed before attaching it to a med line or bifuse. TRUE/FALSE Answer: TRUE 2) You should always wear gloves when hanging a med or flush and when hanging new IVF. TRUE/FALSE Answer: TRUE 3) How often do you need to change your med tubing? a) with every med b) every 24 hours Answer: b c) every 48 hours d) every 72 hours 4) What should you use to clean your patient's PICC LINE during a sterile dressing change? a) Betadine Answer: a b) Alcohol c) Sali wipes d) None of the above 5) Alcohol is used to clean your Broviac Line during a sterile CVL dressing change. TRUE/FALSE Answer:TRUE 6) How long should "Scrub the hub" take before breaking into a line? a) 1 second b) 3 seconds c) 5 seconds Answer: c d) 10 seconds 7) A small circle of Betadine should be left at the insertion site of your PICC/Broviac during a dressing change. TRUE/FALSE Answer: FALSE 8) How often should you change the dead ender/blue clave on the end of a capped CVL or UVC lumen? a) After any blood draw b) After giving blood products c) Every 7 days d) All of the above Answer: d 9) When doing a PICC line dressing change, where should your heart/disc be located? a) Underneath the tegaderm b) Outside of the tegaderm c) Underneath the tegaderm with a chevron. Answer: c d) Outside the tegaderm with a chevron. 10) Who should you contact if your patient has impaired skin integrity related to the tegaderm dressing on a central line? a) the MD only b) the Charge nurse c) the CAT team (Central Access Team) d) Both a and c Answer: d
I- Improve • Use of improvement tools, project management tools, and designing experiments. • We chose PDSA (Plan, Do, Study, Act) • Ran small scale experiments • Captured data • Reported back to group • Used for full scale decision making
I-So what did we do? • Staff education was #1 • Observation Data Collection Tools Created • Using the FMEA, we identified those areas that could be changed quickly at little cost. • Performed small scale experiments (IV fluids in pharmacy) • Decreased variation by sharing proper techniques and monitoring with audits • Changed out dressing change kits to help decrease need for obtaining supplies outside of the sterile field • Established a partnership with the CAT and infection prevention. • Maintenance and Insertion Checklists implemented and monitored • Measured reduction in defects
Track/follow CVL care in OR, how handled and if events occur Review NICU infection control policy General Infection control-OR’s scrub routine vs. current NICU scrub Update CVL P&P if changes identified Follow/track why CVLs discontinued Drsg changes, how done, by whom, when done, migration rate and infection occurrence Chlorohexadine for line changes Tubing change documentation, sticker use Electronic documentation Medication Tubing change every 72 hours vs. every 24 hours Closest port to baby Reduce amount of times lines are accessed New claves/posiflows, impregnated lines, caths etc Hand washing in pharmacy Med. Prep in pharmacy and at bedside TPN/IL/meds under the hood Patient handling and lines- Rad, PT, OT, RT Mechanism that assists with switching from IV to PO meds Order set re; above and for line maintenance NICU CVL dressing team- core group vs. whole unit – “super user” Vanco Hep flushes Hub care Awareness Education on data/stats Utilize on the pot educational sheets Parking lot
C-Awareness Board • Ongoing Meetings • Created public board that showcases: • Number of days since last infection • Tip of the week that is determined at prior meeting