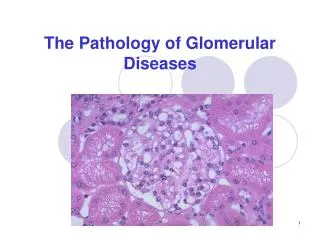
Renal Structure and Function & Urinary Tract I nfections
380 likes | 629 Vues
Renal Structure and Function & Urinary Tract I nfections. Angus Ritchie BPT Lecture Series 2012. Content. Anatomy/Radiology/Function Structure and function of the renal system and male and female genital tract

Renal Structure and Function & Urinary Tract I nfections
E N D
Presentation Transcript
Renal Structure and Function&Urinary Tract Infections Angus Ritchie BPT Lecture Series 2012
Content • Anatomy/Radiology/Function • Structure and function of the renal system and male and female genital tract • Applies basic science knowledge to appreciate the significance of, and appropriately act, on reports of imaging (renal tract ultrasound, functional renal scans, renal angiograms, urograms), renal biopsies, urine composition • Urosepsis / UTI • epidemiology, pathophysiology, clinical presentation, differential diagnosis, • investigations, detailed initial management, principles of ongoing management, potential complications of the disease and its management, • preventive strategies
Urinary tract anomalies • Affects 10% newborns • Kidney • Agenesis, hypoplasia/dysplasia • Fusion (horseshoe), pelvic location • PUJ obstruction • Ureters • Bifid, ectopic (duplex) • Megaureter • Bladder - reflux • Urethra - posterior urethral valves
Normal adult renal anatomy • Kidneys • Size • Men 12.4 ±0.9cm, 202 ±36mL • Women 11.6 ±1.1cm, 154 ±33mL • Right kidney lies lower than left • Retroperitoneal • Age related change • 10% loss of mass per decade after 40y • 10-30% glomerulisclerosed by 80y • Approx 1mL/min/y decline in GFR after 40y
Common normal variants • Accessory renal vessels in 25% • Horseshoe kidney 1 in 600
Autoregulation of RBF, GFR Glomerular filtration, selectivity Tubular transport Tubuloglomerular feedback Countercurrent system Oxygen sensing Pressure sensing Renal sympathetic outflow Electrolyte homeostasis Water homeostasis BP regulation Erythropoiesis regulation Vit D activation Renal physiology (on 1 page)
Renal physiology • Renal blood flow • 1L/min (Approx 20% CO) • Autoregulation (80-180mmHg) • Afferent (PGE2, PGI2) • Efferent (ATII, ET1) • Normal GFR 120mL/min/1.73m2 (wide range)
Renal investigations • Dipstick UA • Urine microscopy, culture • Cells, casts, crystals • Plasma and urine electrolytes • Plasma and urine osmolality • GFR measurement • Urine protein assessment • Acid-base measurement • Renal imaging • Renal biopsy
Renal imaging • Plain xray • Xray KUB • IVP • Ultrasound • CT KUB (multiple phases) • MRI • DTPA/MAG3 • DMSA • PET
Plain imaging • Xray-KUB • IVP • MCUG
Ultrasound • Good tissue definition • cortex, medulla, pyramids, pelvis • Sensitive for obstruction, cysts • Good for antenatal imaging • Poor imaging of • Ureters • Obese patients • Renal vasculature (except transplant)
Renal CT • Better for obese patients • Less sensitive than US for obstruction • Issues with contrast nephropathy • CT-KUB • Stones • Fine calcification • Multiphase CT (non-contrast, arterial, venous, delayed) • Vasculature, vascular lesions, complex cysts • Delayed phase has essentially replaced IVP • CT-angiography for renovascular disease screening
Renal MRI • Excellent for: • Complex masses (necrosis v haemorrhage v fat) • Renal vasculature (with or without contrast) • Best test for renal vein thrombosis • Gadolinium & nephrogenic systemic fibrosis • Only an issue if GFR<30 and multiple studies • Gd can be removed efficiently by haemodialysis • Not rebatable
Renal angiography • Formal angiography the gold standard for RAS • CT insensitive for fibromuscular dysplasia • Allows angioplasty • PCI for atherosclerotic RAS not of proven benefit cf medical therapy • Preoperative embolisation of renal tumours • ?Expanding role for renal artery denervation.
Nuclear renal imaging • Technetium-99m • Used in essentially all nuclear renal imaging • Emits gamma rays, half-life 6h • Nuclear GFR • 99mTc-DTPA or 51Cr-EDTA (5% difference) • DTPA, MAG3 • Renal perfusion, uptake, excretion, drainage • MAG3 better if impaired renal function, obstruction • Lasix optional • DMSA (to look at the ‘meat’) • Acute pyelonephritis • Cortical scarring
Cystoscopy • Good for investigation of haematuria • Especially macroscopic haematuria • Allows retrograde imaging • Defines location of obstruction • Diagnosis of radiolucent stones (eg indinivir)
Urinary tract infections • Common • Wide spectrum of disease • Mild, community treated • Fatal septic shock
Common UTI organisms • E. coli • Proteus mirabilis • Klebsiella spp. • Enterococci • Group B Strep. • Other gram –ves
UTI Confirmation • UA • Positive leucocytes (false –veVitC, protein, glucose, AB) • Positive nitrites (most Gram –ves) • Small blood, protein common • Urine microscopy • Pyuria WC 10-100 • Organisms • No epithelial cells • Culture • Pure growth >10^7 CFU • Bacteraemia = pyelonephritis
Role of imaging in UTI • NOT REQUIRED FOR DIAGNOSIS • Rule out obstruction • Old men • Associated with ARF • History of stones • Failure to respond to Rx • ?Abscess or lobar nephronia • Recurrent infections • ?Renal scarring or bladder dysfunction • Stranding on CT is ENTIRELY NON-SPECIFIC
Childhood UTIs • Common • 8% of girls, 2% of boys <7y • 10-30% have recurrent infection • Similar organisms to adults • DMSA sensitive test for pyelonephritis • May indicate VUR • Screening with US, MCUG highly recommended for febrile UTI <2y. • ?Role of circumcision (NNT 111)
Cystitis • Often urine culture not required • Treatment • Trimethoprim, cephalexin, amoxy+clav • Women: 3-5 days • Men: 14 days. Look for anatomical abnormality
Pyelonephritis • Blood and urine cultures before treatment • Antibiotics • IV AB until afebrile, then orals. Complete 10-14d • Empirical AB depends on local epidemiology • Cephazolin + gentamicin • Repeat urine culture 48h after Rx • If not improving look for abscess • Areas of lobar nephronia are considered antecedent of abscess and require extended treatment. • Oral quinolonesexcellent penetration of renal tissue but overuse associated with resistance
Pyelonephritis in Pregnancy • Must be treated seriously - can cause ARF • Mild hydronephrosis (esp R sided) is common and not indicative of obstruction • Repeat urine culture 48h post treatment
Pyelonephritis in Transplant • Mimics acute rejection • Fever • Graft tenderness • ARF • Look for suggestive UA, urine micro • Imaging mandatory to rule out obstruction • Treat aggressively, prone to shock
Catheter-associated UTI • Bacterial colonisation inevitable • Only symptomatic infections require Rx • Use broad-spectrum AB • May respond to Rx even if organism is resistant • Lower rate of infection with SPC • Catheter change with symptomatic infections • With antibiotic cover • Routine catheter changes
UTI prophylaxis • Recurrent UTI (2 or more in a year) • Evidence of benefit in non-pregnant women if taken for 6-12 months (Cochrane Review) • Intermittent self-treatment • Intermittent prophylaxis (eg post-coital) • Continuous • Options • Cephalexin 250mg nocte • Trimethoprim 150mg daily
UTI prevention • Good urine volume • Urinary acidification • Sodium citrate (Ural) • Cranberry tabs (in women)* • Topical estrogens (postmenopausal women)* • Hexamine hippurate* • Double-voiding (men with prostatism) • Or intermittent self-catheterisation * Evidence based benefit on Cochrane review
Prostatitis • Disease of older men • Presentation: • Lower urinary tract symptoms • Perineal pain • Fever • Prostatic tenderness • 2-4 weeks Rx. Quinolones a good choice. • Check for Chlamydia in young men
Asymptomatic findings • Asymptomatic bacteriuria • In general no Rx required • Exceptions: pregnant women, before procedures • Asymptomatic Candiduria • Remove catheters, stents • Treat only high risk patients • Asymptomatic pyuria
Random tips • Stones and UTI - associated with Proteus spp. • Old men - always look for urine retention • Emphysematous pyelonephritis associated with diabetes. • Increasing community prevalence of ESBL