Download
1 / 1
10 likes | 200 Vues
2005 HIV Diagnostics Conference Orlando, FL February 28-March 1, 2005. 2005 APHL Infectious Disease Conference Orlando, FL March 2-4, 2005. METHOD COMPARISON OF HIV TESTS FOR RECENT INFECTION

E N D
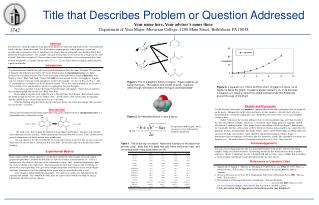
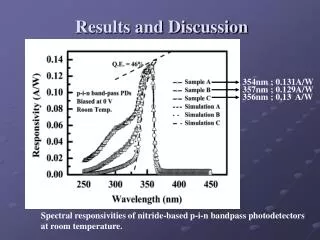
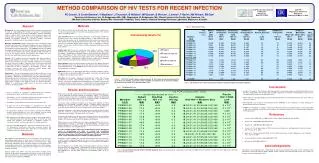
2005 HIV Diagnostics Conference Orlando, FLFebruary 28-March 1, 2005 2005 APHL Infectious Disease Conference Orlando, FLMarch 2-4, 2005 METHOD COMPARISON OF HIV TESTS FOR RECENT INFECTION PE Garrett1, S Crush-Stanton2, V MacKeen2, J Thurston2, B Weiblen2, MP Busch3, B Werner4, J Jenner4, F Barin5, KM Wilson6, EM Dax6 1SeraCare Life Sciences, Inc., W. Bridgewater, MA; 2BBI Diagnostics, W. Bridgewater, MA; 3Blood Centers of the Pacific, San Francisco, CA; 4MA State Laboratory Institute, Boston, MA; 5Université F Rabelais, Tours, France; 6National Serology Reference Laboratory, Melbourne, Australia Abstract Background: Accurate laboratory assessment of incidence vs. prevalence or early vs. long-standing HIV infection is valuable for epidemiological studies and for diagnostic assessment of individuals. We have completed a study of samples from a large group of deferred plasma donors with unknown dates of HIV infection using several candidate HIV incidence test methods to categorize samples as ‘consensus incident’, ‘consensus prevalent’ or ‘lacking consensus’ by a variety of methods. Materials and Methods: Samples tested were from a repository of well-characterized plasma units from deferred donors who were confirmed HIV positive. HIV incidence test methods included less-sensitive, avidity index, and methods using novel approaches. The PRB601 panel was assembled by aliquoting samples from units that tested incident or prevalent by at least 11 of the 12 test methods used, and by preparing a data sheet with test results for HIV markers and for nine incidence test methods (four less-sensitive, two avidity index, and three other approaches). Results: Of 78 samples tested by 12 methods, 42% were prevalent or long-standing infection by all methods. Only 6% were incident or recent infections by all methods, but if one candidate method was not considered, 18% were consensus incident. There was a lack of consensus (more than one method in disagreement with others) in 29% of this sample set, some of which may be due to variations in the definition of recent. Eight consensus prevalent and seven consensus incident samples were assembled into a panel for evaluating incidence tests. Conclusions: A clear understanding of HIV incidence (the rate of new infections) is important for formulating health care policy and efforts to fight the epidemic. Although long seroconversion series (that would constitute a gold standard) do not currently exist, useful information can be derived from samples with unknown seroconversion dates if consensus results are found from multiple incidence test methods based on different principles. PRB601 is a commercially available panel of consensus incident and consensus prevalent samples. Methods HIV incidence methods described to date have all involved measuring differences in immune responses between recent and long-standing infections. The methods can be classified as below: Less Sensitive (LS): these tests involve ‘de-tuning’ a commercially available HIV method to make it less sensitive by diluting samples, so that samples from early infection (that are positive on the unmodified test) will be below a specified cutoff, while samples from long-standing infection will be above the cutoff. Results are expressed as Standard Optical Density (SOD) using a calibrator to normalize results. LS tests were the first incidence methods developed, and have been the most studied.1,2 Avidity Index (AI): these tests exploit the lower avidity of early vs. ‘mature’ antibodies for the target HIV protein antigens. In AI methods, the sample is split: one aliquot is treated with a chaotropic agent in buffer and the other with buffer alone. Both aliquots are then tested using a commercially available anti-HIV test method, and ODs are compared using a ratio expressed as a percentage of treated to untreated sample. Early infection samples will have a lower ratio, as antibody-antigen complexes will have been disrupted by the chaotropic agent.3,4 Novel epitopes: these tests detect antibody responses to HIV epitopes that have been empirically found to be expressed in early infection more intensely than in long-standing infection. In the HIV-RI method, results are expressed as mean OD and compared to a calibrator.5 BED-CEIA: this test is an IgG-capture EIA where increasing proportion of gp41-IDR specific Abs are detected by BED-biotin peptide. Results are normalized using a calibrator OD and expressed as OD-n.6 NRL HIV-1: this test identifies individuals infected with HIV-1 within 120+/-16 days by detecting a specific antigen-antibody interaction that is transient in recent infection. Results are quantified using a standard curve, and values >20 ug/ml are considered indicative of early infection. To identify HIV-1 infected individuals prior to day 30, this assay must be performed in parallel with a p24 antigen assay.7 Table 2. HIV Incidence Tests Figure 1. Of 58 HIV-1 positive deferred plasma donors, 28 (48%) were classified as prevalent by all or all but one method, and 10 (17%) were classified as incident by all or all but one method. No consensus was found for 20 deferred donors (34%). Table 2. HIV incidence test results on final panel members sorted by incident or prevalent categories. • Conclusions • A study of 78 samples from 58 donors with unknown HIV seroconversion dates has demonstrated that the Less Sensitive, Avidity Index, HIV-RI, BED CEIA, and NRL approaches to incidence testing produce results that are consistent with one another in the majority of cases. • Further analysis of the data taking into account differing definitions of recent infection may resolve some of the ‘no consensus’ samples. • BBI Diagnostics has produced a Performance Panel (PRB601) for the evaluation of newly developed or implemented incidence test methods. • PRB601 has 15 members, including 7 consensus incident and 8 consensus prevalent samples, and is supplied with a data sheet containing results from nine incidence test methods performed in five internationally recognized referee laboratories. Table 1. HIV Diagnostic Tests • Introduction • Tests for incidence vs. prevalence of HIV infection are needed by epidemiologists, public health professionals and researchers. • Policymakers use the information generated to answer questions like “Are current efforts to slow the HIV epidemic effective?” • Distributions of funds depend on the answers to these questions. • To date, no test for HIV incidence vs. prevalence has won wide acceptance, but a number of candidate methods have been developed. • To evaluate these methods, series of samples collected from individuals recently infected through the first year following infection would constitute ‘gold standards’, but such series are extremely rare. • BBI organized an international study of samples from a large group of U.S. deferred plasma donors with unknown dates of HIV infection using several HIV incidence test methods to categorize samples as ‘consensus incident’, ‘consensus prevalent’, or ‘lacking consensus’. • From this study, BBI Diagnostics, a division of SeraCare Life Sciences, Inc. developed a Performance Panel with consensus incident and consensus prevalent samples and a data set to assist developers and evaluators of tests for recent HIV infection. Results and Discussion Results from testing 78 samples from 58 HIV-1 positive deferred plasma donors by 12 tests employing 10 different methods are illustrated in Figure 1. Of 58 donors, 25 had consensus results (43%, 21 prevalent, 4 incident). Another 13 donors had consensus results on all but one test (22%, 7 prevalent, 6 incident). Twenty donors (34%) had one or more units in the ‘no consensus’ category. Consensus results (incident or prevalent by all tests) were obtained for 38/78 samples (49%, 33 prevalent, 5 incident). Another 17 samples had the same result for all but one test (22%, 8 prevalent, 9 incident). ‘No consensus’ was defined as more than one discrepant result, and 23 samples (29%) fell into this category. Seventeen same-donor series were collected over short periods of time (2-9 days, mean 4.3, median 3), so plasma units from the same donor might be expected to fall into the same category. This was true for 14/17 donors. In summary, 38 samples from 25 donors had consistent results by all test methods, and 55 samples from 38 donors had results consistent by all or all but one test method. No consensus was found for 23 samples from 20 donors. Where consensus was lacking, one cause may be varying definitions of recent vs. long-standing or incident vs. prevalent for different methods. Defined ‘recent’ intervals ranged from <120 days to <279 days for different methods, and for some methods the interval is still being determined. Accurate estimates of HIV incidence do not depend on a specific definition of recent vs. long-standing, but rather on accurate and reproducible discrimination between the two categories, whatever the cutoff. If continued experience demonstrates that different methods have different discrimination points, useful information may be available from both approaches. Performance Panel PRB601 was assembled from samples that had consensus results (7 incident, 8 prevalent) with at least 11 of 12 tests. Characteristics of the panel members and data from several incidence test methods are described in Tables 1 and 2. One HIV diagnostic test showed some discrimination between consensus incident and consensus prevalent samples. HIV antigen was positive for three consensus incident samples in PRB601, and negative for all consensus prevalent samples. HIV antibody tests and HIV RNA showed no discriminatory power at all, as expected. • References • Janssen et al. JAMA 1998 Jul 1;280(1):42-8: Erratum: JAMA 1999 May 26;281(20):1893. • Kothe et al. JAIDS 2003 Aug 15;33(5):625-34. • Suligoi et al. JCM 2002 Nov;40(11):4015-20. • Jenner et al. Poster presentation at 10th Conference on Retroviruses and Opportunistic Infections, Boston, MA, February 10-14, 2003. • Barin et al. Poster presentation LB21 at The 2nd IAS Conference on HIV Pathogenesis and Treatment, Paris, July 13-16, 2003. • Hu et al. AIDS Res and Hum Retro 2003;19:727-730. • Wilson et al. AIDS 2004;18:2253-9. Materials BBI supplied to nine laboratories a set of 78 samples from plasma units representing single bleeds or short series (2-3 bleeds) from 58 HIV-1 positive deferred plasma donors with unknown seroconversion dates. Eight laboratories supplied test results for twelve incidence test methods in time for preparation of this poster. One laboratory did not receive three samples, and one laboratory was not able to test five samples for one of the two methods it reported. Plasma samples from fifteen units that tested either ‘incident’ (recent infection) or ‘prevalent’ (long-standing infection) by at least 11/12 methods were developed into a commercially available HIV-1 Incidence/Prevalence Performance Panel (BBI Panel PRB601). Acknowledgements The authors are most grateful to Dr. Yiping Zhang for advice and assembly of the poster, and to collaborators and data donors Joanne Mei, Michele Owens, Bharat Parekh, Thomas Folks and Ron Otten of the U.S. Centers for Disease Control and Prevention (CDC) . Table 1. Characterization of panel members with HIV diagnostic tests. A preliminary panel configuration presented at CVS 2004 has been modified. The data here and in Table 2 were collected on the final panel members.