Study method
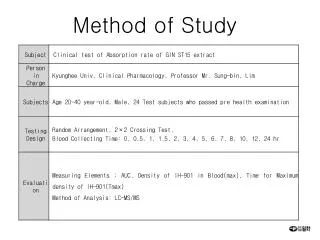
Study method. Method. Data collection during month of June 2003 Patients ≥ 16 years of age admitted to a general ICU regardless of outcome Patients identified by hospital and questionnaires circulated by hospital (local reporter or other contact within ICU)

Study method
E N D
Presentation Transcript
Method • Data collection during month of June 2003 • Patients ≥ 16 years of age admitted to a general ICU regardless of outcome • Patients identified by hospital and questionnaires circulated by hospital (local reporter or other contact within ICU) • Two questionnaires for each case – physician and intensivist
Method (cont) • Quantitative and qualitative analysis • Multi-disciplinary advisor groups • Intensivists – both medical and anaesthetic background • Physicians • Nurses
Consultant physician involvement • 439 sets of notes reviewed • Good data only obtainable in 40 cases • 23 of 40 patients reviewed within 24 hours (58%) • 28 patients with ward stay >24 hours prior to ICU • 11 of 28 reviewed within 24 hours (39%)
Physiological derangement • Cardiorespiratory arrest • Respiratory rate: <8 or >30 breaths per minute • Sa02 <90% on oxygen • Difficulty speaking • Pulse rate: <40 or >130 beats per minute • Systolic blood pressure <90mmHg • Repeated or prolonged seizures • Any unexplained decrease in consciousness • Agitation or delirium • Concern about patient status not detailed above
Duration of instability Time between first physiological instability and referral to ICU Patients that were in hospital for more than 24 hours prior to ICU admission Patients that were in hospital for 24 hours or less prior to ICU admission
Key findings • The quality of the initial hospital admission history and examination was acceptable in 90% of cases. • Despite an acceptable history and examination, initial treatment was often delayed, inappropriate or both. • Consultant physician involvement in first 24 hours low.
Key findings (cont) • Of the patients who had been in hospital more than 24 hours prior to ICU admission, 66% exhibited physiological instability for more than 12 hours.
Recommendations • Trusts should ensure that consultant job plans reflect the pattern of demand of emergency medical admissions and provision should be made for planned consultant presence in the evenings (and perhaps at night in busier units). • A consultant physician should review all acute medical admissions within 24 hours of hospital admission.
Recommendations (cont) • Trusts should ensure that consultant physicians have no other clinical commitments when on take. This may be through the development of acute physicians. This will allow for greater involvement in the assessment and treatment planning of new admissions and the review of deteriorating inpatients. • More attention should be paid to patients exhibiting physiological abnormalities. This is a marker of increased mortality risk. • Robust track and trigger systems should be in place to cover all inpatients. These should be linked to a response team that is appropriately skilled to assess and manage the clinical problems.
Key findings • Notes seldom contained written requests regarding the type and frequency of physiological observations. • Instructions giving parameters that should trigger a patient review were rarely documented. • Respiratory rate was infrequently recorded • 27% of hospitals did not used an early warning system.
Recommendations • A clear physiological monitoring plan should be made for each patient. This should detail the parameters to be monitored and the frequency of observations. • Part of the treatment plan should be an explicit statement of parameters that should prompt a request for review by medical staff or expert multidisciplinary team.
Recommendations (cont) 3. The importance of respiratory rate monitoring should be highlighted. This parameter should be recorded at any point that other observations are being made.
Key findings • A high percentage of patients were referred to critical care by staff in training. 21% of referrals were made by SHOs. • Consultant physicians had no knowledge or input into 57% of referrals to critical care. • Delays between referral to critical care and review (5%) and between decision to admit to critical care and admission (16%) were common. • A significant factor in delay was the lack of appropriate staff and ICU beds. • 18% of patients were admitted to ICU without prior review by the intensive care service.
Recommendations • Consultant physicians should be more involved in the referral of patients under their care to ICU. • It is inappropriate for referral to ICU and acceptance to ICU to happen at SHO level. • Any delay in admission to critical care should be recorded as a critical incident through the appropriate hospital incident monitoring and clinical governance system. • All inpatient referrals to ICU should be assessed prior to ICU admission. Only in exceptional circumstances should a patient be accepted for ICU care without prior review.
Frequency distribution of time of ICU admission Day: 08:00 - 17:59 Evening: 18:00 – 23:59 Night: 00:00 – 07:59
Time to consultant review Proportion of patients reviewed by an intensivist Time since ICU admission (Hours)
Key findings • Evening (18:00 – 23:59) was the busiest time for new medical admissions to ICU, followed by night (00:00 – 07:59) and lastly day (08:00 – 17:59). • One in four patients were admitted to the ICU without consultant intensivist involvement. • Amongst the 40% cases for which data were available, approximately one in four patient were not reviewed by a consultant intensivist within 12 hours of admission
Recommendations • Trusts should ensure that consultant job plans reflect the pattern of demand for emergency admission to ICU and provision should be made for planned consultant presence in the evenings (and perhaps at night in busier units). • Patients should rarely be admitted to ICU without the prior knowledge or involvement of a consultant intensivist. • A consultant intensivist should review all patients admitted to ICU within 12 hours of admission. Regular audit should be performed against this standard.
Was ICU admission avoidable? Different care could have prevented need for admission – 21 cases • Treatment limitation decision could have avoided admission – 58 cases
Assessment of clinical care • Airway • Breathing • Circulation • Monitoring • Oxygen therapy
Airway Management 90 80 70 60 50 40 30 20 10 0 1 2 3 4 5 6 7 8 9 Very Poor Excellent Scale
Assessment of clinical care - poor • Airway 11% • Breathing 16% • Circulation 14% • Monitoring 13% • Oxygen therapy 14%