Augmentative and Alternative Communication Usage in Canadian Children: A Comprehensive Study
20 likes | 136 Vues
This study explores the characteristics and effectiveness of Augmentative and Alternative Communication (AAC) systems among Canadian children with developmental disabilities. Through two studies—quantitative parent surveys and qualitative interviews—findings reveal significant variations in AAC system usage, demonstrated communication levels, and the impacts of adaptive and maladaptive behaviors. Approximately 50% of children showed improved communication with AAC, while others faced communication barriers. The research highlights the need for tailored AAC interventions and more supportive services during AAC transitions.

Augmentative and Alternative Communication Usage in Canadian Children: A Comprehensive Study
E N D
Presentation Transcript
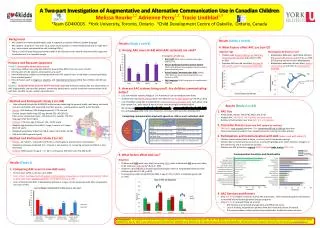
A Two-part Investigation of Augmentative and Alternative Communication Use in Canadian Children Melissa Rourke1,2 Adrienne Perry1,2 Tracie Lindblad1,3 1Team GO4KIDDS 2York University, Toronto, Ontario 3Child Development Centre of Oakville, Ontario, Canada No Benefit ~50% * Benefit ~50% * Background • Background • AAC systems are methods/techniques used to augment or replace children’s spoken language • AAC systems range from “low-tech” (e.g., basic yes/no systems, or velcro-backed pictures) to “high-tech” (e.g., voice output communication aids including iPADs) • There is a lack of empirical group-based studies in the literature and a need to document AAC usage and its effectiveness in a Canadian sample Results (Study 1 cont’d) 4. What factors affect AAC use (con’t)? Results (Study 1 cont’d) 2. Among AAC users (n=63) what AAC system(s) are used? • Adaptive Age • Children with a lower adaptive agehad lower levels of communication with AAC (F=5.99, p=.001) • Adaptive skill level did not affect: the type of AAC system used, or improvement with AAC • Maladaptive Behaviour Level • Maladaptive behaviour significantly affected the type of AAC system used(F=3.11, p=.034) (PECS group had most severe Maladaptive) • Maladaptive behaviour did not affect: level of communication with AAC, or improvement with AAC • 4 Categories of AAC use: • Basic AAC (24%): yes/no switches, basic signs, gestures, etc., • Picture Exchange Communication System (PECS; 32%): Bidirectional exchange of pictures with a communicative partner • Voice Output Communication Aids (VOCAs; 14%): Electronic speech generating devices, e.g., Dynavox or iPADs • Sign language(31%): Using signs as a sophisticated language • Purpose and Research Questions • Study 1. Quantitative Parent Online Survey • How many children are using AAC systems? How do they differ from non-users of AAC? • Among users of AAC systems, what systems are used? • How effectively do children communicate with their AAC system? Does it help them communicate better than unaided speech? • How do factors such as diagnosis, adaptive, and maladaptive behaviour affect how children with DD use AAC? • Study 2. Qualitative Study based on Parent Interviewsexploring themes including:AAC use, experiences of AAC longitudinally, the transition process, community participation, specific functional communication skills with AAC, and AAC service system issues/barriers • 3. How are AAC systems being used? Are children communicating better? • 29% use multiple systems (Range of 1 to 4 systems in use currently/at same time) • Children who used VOCA systems were more likely to use multiple systems(χ 2=10.44, p=.015) • 53%of children using AAC are reported to communicate at a very basic leveleven when using their system (i.e., basic needs & wants or very little meaningful communication) • We compared communication level with speech to communication level with AACfor each individual child. Only 50%showed an increased communication level/benefit! • Method and Participants Study 1 (n=148) • Datacollected through the GO4KIDDS online survey examining the general health, well-being, and social inclusion of children with severe DD, and their parents – used questions specific to SLP and AAC • Parents: 95% mothers, 92% biological parents, 77% married • Diverse sample (wide range SES avg. Barratt SES = 40 (SD=13) from across Canada (see map); 23% not born in Canada, 17% first language other than English • Children: 71% boys; age 3-19 years (M = 10.91 years) • Adaptive Age Equivalent from SIB-R: range 3 months to 13 years (M=3.25 years) • Maladaptive Behavior Index from SIB-R: range -56 to 4 (M=-15.90) • 55% with ASD (by parent report) • Method and Participants Study 2 (n=12) • Parents: all mothers, recruited from Study 1, private agency, special school, and websites • Telephone interview conducted (1.5 -2 hours) in two sessions (1. screening, consent and SIB-R; 2. AAC interview) • Children:58% boys (n=7); age 4 – 17 (M = 11.33 years); 25% DD (n=3), 75% ASD (n=9) • Results (Study 2; n=12) • 1. AAC Use • Primary AAC: VOCAs: 75% (n=9); PECS: 25% (n=3) • Multiple AAC: 42% (n=5; 1 to 4 systems currently in use) • Number of AAC systems over time: (M = 3; 1 to 5 systems) • 2. Transition Process (from one AAC system to another) • 50% (n=6):easy or good transition, 50%:somewhat difficult or difficult transition. • Parents expressed a need for more supportive services during transition process • 3. Participation and Communication with AAC (where and with whom?) • Children communicated best at home, in school, and in therapeutic settings. • Children did not communicate as much or as well with grandparents, other relatives, strangers, in the community, and at recreational activities. • Children use AAC primarily to request83% (n=10) and make choices75% (n=9) • 4. AAC Services and Barriers • Only 33% (n=4) children received a formal AAC assessment, other families bought for themselves, or received informally through other therapy programs • Only 50% (n=6) received follow-up services • AAC Services are fractured, disorganized, and difficult to access • Lack of funding, long waitlists (parents often don’t wait and pay out of pocket) • Disconnect between school system and private/public healthcare system services Comparing communication level with speech vs. AAC in each individual child Communicative Functions and Participation • 4. What factors affect AAC use? • Diagnosis • Children with ASD were more likely to be using PECS, while children with DD were more likely to be using Sign language(χ 2=8.43, p=.038) • Children in the ASD group showed significantly higher levels of maladaptive behaviour than children with DD (F=7.86, p=.007) • The two groups did not significantly differ in age (F=.01, p=.937), or adaptive age (F=.08, p=.783) School Home Community Clinical Settings • Results (Study 1) • 1. Comparing AAC users to non-AAC users • 63 AAC users (42%) vs. 85 non-users (58%) • Users of AAC had lower levels of spoken communication, measured on a 4-point ordinal scale (χ2=20.62, p<.001), AND lower adaptive skill levels on the SIB-R (t=2.04, p=.04). • Users of AAC did not differ in Maladaptive behaviour or age, nor the proportion with ASD, compared to non-users of AAC * * Acknowledgments: We would like to thank all the families who completed the Surveys and interviews for this study. We are very grateful to Teresa Lee for her assistance with recruitment and data collection and Azin Taheri for her assistance with the GO4KIDDS data. Data for Study 1 were collected as part of the CIHR Team: GO4KIDDS: Great Outcomes for Kids Impacted by Severe Developmental Disabilities, Nominated Principal Investigator: Adrienne Perry, York University. (www.go4kidds.ca)