Download
1 / 45
750 likes | 1.64k Vues
CNS PHARMACOLOGY. FARIBORZ KEYHANFAR Ph.D, D.I.C TUMS - Department of Pharmacology. 238 SLIDES. First to be discovered by humans How Long. 100 yrs ? 500 yrs ? 1000 yrs? 2000 yrs ? Ever since the beginning of written history: Cave Walls, Bible, Torah, Koran, mind altering

E N D
CNS PHARMACOLOGY FARIBORZ KEYHANFAR Ph.D, D.I.C TUMS - Department of Pharmacology 238 SLIDES
First to be discovered by humansHow Long 100 yrs ? 500 yrs ? 1000 yrs? 2000 yrs ? Ever since the beginning of written history: Cave Walls, Bible, Torah, Koran, mind altering mood altering
Higher number of synapses networks of inhibitory Neurons Use of more than 10-50 NT’s Only 2 NTs
Neurotransmitters affect targets by acting on receptors – protein molecules in the postsynaptic membrane Ionotropic receptors are fast – open an ion channel when the transmitter molecule binds Metabotropic receptors are slow – when activated alter chemical reactions in the cell, such as a G protein system, to open an ion channel
Nerve cells membrane contain two types of channels Defined on the basis of the mechanisms controlling their Opening and closing A ligand is a substance that binds to a receptor حساس به لیگاند NT Na channel Heart FAST یونوتروپیک حساس به تغییرات ولتاژ سلول متابوتروپیک SLOW پروتئین G پیامبرهای ثانویه
Receptor Types There are 3 subclasses of membrane receptors: 1. channel linked receptors – ion channel that opens in response to a ligand 2. enzymatic receptors – receptor is an enzyme that is activated by the ligand 3. G protein-coupled receptor – a G-protein (bound to GTP) assists in transmitting the signal
ROLE OF THE ION CURRENT CARRIED BY THE CHANNEL SYNAPSE- communication EPSPs - Ionotropic receptor Stimulation of excitatory neurons causes a movement of ions that results in a depolarization of the postsynaptic membrane. IPSPs - Presynaptic inhibition Stimulation of inhibitory neurons causes movement of ions that results in a hyperpolarization of the postsynaptic membrane.
Where Does Diffusion Take the Ion? Na+ 150 mM K+ 5 mM Cl- High Exterior I N O UT I N Interior Na+ 15 mM K+ 150 mM Cl- Low
Ion Diffusion • Key to neurophysiology • Dependent upon: • Concentration gradient • Electrical gradient • Modified by: • ‘Gated ion channels’
Are You Ready for a Big Surprise? Many CNS drugs act on GABA receptors to effect the frequency and duration of action potentials!
HOW DRUGS WORK General anesthetics andalcohols via nonspecific actions on membranes?? Non-specific Direct interaction with molecular components of ion channels on axons Carbamazepine Phenytoin
HOW CNS DRUGS WORK Drugs in CNS act on specific receptors mainly at the synapses Specific Receptor Drug
Treatable NT diseases Action potential Drugs are developed that address these 9 steps as an : Activate - AGONIST (mimic the NT ) Block - ANTAGONIST (the NT) E E E E I I E E I GAS nitric oxide (NO) Most drugs that act on the CNS do so by changing ion flow through transmembrane channels of nerve cells Ion channel opens : cAMP, IP3 … activation :
Drug Action on Synaptic Transmission Agonist drugs are in red, Antagonists are in blue
Central neurotransmitters • Amino acids • Neutral amino acids – Glycine & GABA • Acidic amino acids - Glutamate • Acetylcholine • Monoamines • Dopamine • Norepinephrine • 5-hydroxytryptamine • Peptides – Enkephalins, Endorphins, SubP, VIP, TRH, Neurotensin, Neuropeptide Y, … • Nitric oxide • endocananbiniods
Two main classes of monoamine neurotransmitters: • Catecholamines – dopamine (DA), epinephrine, norepinephrine (NE) • Indoleamines – serotonin (5-HT), melatonin Receptor subtypes – the same neurotransmitter may bind to a variety of subtypes, which trigger different responses DA1, DA2, DA3, DA4, DA5 Endogenous – occurs naturally within the body: Endogenous ligands– substances that the brain produces (neurotransmitter) Exogenous – introduced from outside the body in opiates, endorphin/enkephalin vs. morphine
GABA receptors are in 3 classes: • GABAA - ionotropic, producing fast, inhibitory effects – Opens Cl ion channels S-H BDZs, Barbiturates, Zolpidem Gabapentin, tiagabine, vigabatrin Influence GABAA • GABAB - metabotropic, slow inhibitory effects through neurogliaform interneurons – activated by Baclofen (a centrally acting muscle relaxant) coupled to G proteins , open K channels or close Ca channels • GABAC- ionotropicwith a chloride channel
4 Neurotransmitter Systems Form a Complex Array in the Brain Two types of ACh receptors: • Nicotinic – most are ionotropic and excitatory Example: muscles use nicotinic ACh receptors – paralysis can be induced with an antagonist, such as curare • Muscarinic – are metabotropic and can be excitatory or inhibitory Muscarinic ACh receptors can be blocked by atropine or scopolamine to produces changes in cognition.
4 Neurotransmitter Systems Form a Complex Array in the Brain The gas,nitric oxide (NO), differs from other neurotransmitters: • produced in locations other than axon terminals – mainly in dendrites, and diffuses as soon as it is produced, rather than released • diffused into the target cell and to activate cyclic GMP • to serve as a retrograde transmitter by diffusing back into the presynaptic neuron
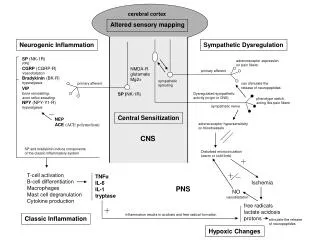
Treatable NT diseases TOO Many NT NT molecules binding to postsynaptic receptors PSYCHOSES Therapy : admin antagonists TOO Much NT A focus of hyperexcitable neurons fire in the absence of appropriate stimuli EPILEPSY Therapy : reduce the automaticity of these cells
Treatable NT diseases TOO little NT Too few NT molecules binding to postsynaptic receptors DEPRESSION – PARKINSONISM Therapy : Treatment strategies (increase NT)
(drug abuse) • Broad definition of drug abuse: Unreasonable administration used in ways that are not medically approved Cause feelings of : Euphoria or alter perception
Drug dependence Person’s reliance on or need to take a substance psychological dependence psychic dependence - Drug use becomes compulsive Addiction emotional reliance to maintain a sense of well-being physiological dependence – physical dependence Dependence
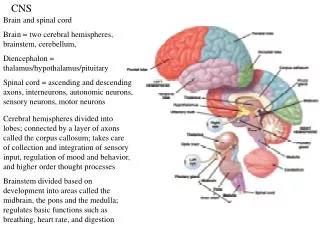
CNS PharmacologyNeurodegenerative Diseases Group of disorders characterized by neuronal loss and generally an accumulation of insoluble intracellular or extracellular material in certain brain regions Most are of unknown etiology : 1.affect the elderly 2.progressive 3.damage selected neuronal populations or brain regions
CNS PharmacologyNeurodegenerative Diseases Some forms of these disorders are inherited most are sporadic occurrences (idiopathic) with risk factors: genetic predisposition environmental factors aging
Neurodegenerative Disorders Alzheimer’s : neural injury is primarily in the hippocampus Parkinson’s : loss of nigrostriatal dopamine neurons Huntington’s : loss of a specific subset of striatal neurons Amyotrophic lateral sclerosis (ALS) degeneration od spinal, bulbar and cortical neurons
Parkinson's Disease FARIBORZ KEYHANFAR Ph.D, D.I.C Degeneration of the darkly pigmented dopamine neurons in the SN Loss of dopamine in the neostriatum Presence of intracellular inclusion bodies (Lewy bodies)
1% over the age of 65 10 % under age 40. four million patients worldwide,
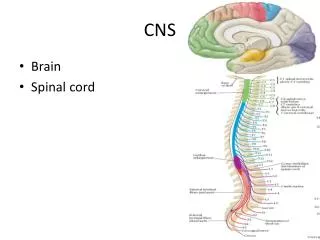
I E Basal Ganglia
James Parkinson 1817 "An Essay on the Shaking Palsy," existed for many thousands of years India as early as 5000 BC, Chinese medical 2500 years ago. no cure Drugs Only treat symptoms • Mech of degeneration of dopamine neurons are not known. Hypotheses : oxidative stress and excitotoxicity
Etiology • Cerebral atherosclerosis • Viral encephalitis • Side effects of several antipsychotic drugs (i.e., phenothiazides, butyrophenones, reserpine) Environmental factors and neurotoxins • Pesticides, herbicides, industrial chemicals - contain substances that inhibit complex I in the mitochondria
Treatment of Parkinson Disease • Levodopa & Carbidopa: increase brain dopamine levels • 2. Dopamine agonists : stimulate dopamine receptors • Bromocriptine - pergolide – Pramipexole – Ropinirole • 3. Catechol-O-methyltransferase inhibitors: increase conc of brain dopamine • Tolcapone – Entacapone • 4. MAO inhibitors : prevent dopamine metabolism - Selegiline • 5. Anticholinergic agents : reduce the excitatory activity within the striatum • Benztropine -Trihexyphenidyl – Biperiden - Procyclidine • 6. Blocking the uptake and enhancing the release of dopamine - Amantadine • 7. Stimulating the release of dopamine - amphetamine • 8. Diphenhydramine (Benadryl)
Dopamine and Tyrosine Are Not Used for Parkinson Disease Therapy • Dopamine Doesn't Cross the Blood Brain Barrier • Huge amount of tyrosine decreases activity of rate limiting enzyme Tyrosine Hydroxylase That normally Converts Tyrosine to dopamine by overwhelming enzyme tyrosine hydroxylase, has a feedback loop that will turn off tyrosine hydroxylase
Effects of L Dopa on the Symptoms of Parkinson Disease • L Dopa Fairly Effective in Eliminating Most of the Symptoms of Parkinson Disease • Bradykinesia and Rigidity Quickly Respond to L Dopa • Reduction in Tremor Effect with Continued Therapy • L Dopa less Effective in Eliminating Postural Instability and Shuffling Gait Meaning Other Neurotransmitters Are Involved in Parkinson Disease
Effects of L Dopa on Behavior • In Terms of Behavior, L Dopa Partially Changes Mood by Elevating Mood, and L Dopa Increases Patient Sense of Well Being • Significant Number of Patients Get Behavior Side Effects
L Dopa- Pharmacokinetics • L Dopa is readily absorbed from GI Tract • Usually large doses must be given since ~1% actually cross Blood Brain Barrier enters CNS • Large amount of L Dopa has to be given due to First Pass Effect • L Dopa metabolized by dopa decarboxylase in liver and periphery to dopamine • Secreted in urine unchanged or conjugated with glucoronyl sulfate • Most of L Dopa converted in periphery to NE and EPI
Levodopa and Carbidopa L- DOPA REPLACEMENT THERAPY 100, 250, 500 mg Does not cross BBB – NO CNS EFFECTS. Is transported into the brain by amino acid transport systems and is converted to dopamine by : L-aromatic amino acid decarboxylase L-aromatic amino acid decarboxylase in the liver, kidneys and GIT metabolize levedopa. Coadmin with Carbidopa (Sinemet) 10:1 Carbidopa is a peripheral decarboxylase inhibitor Blocks GI and peripheral tissue metabolism of DOPA to dopamine (by blocking DOPA decarboxylase) since it does not pass the blood-brain barrier, it does not block dopamine synthesis in CNS
Wearing – off effect increase dose, decrease dose frequencyOn – off effect small doses, higher frequency + bromocriptine Levodopa Anorexia, nausea and vomiting
Catechol-O-methyltransferase (COMT) inhibitors Tolcapone (Tasmar) and Entacapone (Comtan) • Increases the duration of effect of levodopa dose • Can increase peak levels of levodopa • Should be taken with carbidopa/levodopa (not effective used alone) • Can be most beneficial in treating "wearing off" responses • Can reduce carbidopa/levodopa dose by 20-30%
Tolcapone or Entacapone • Block catecholamine-O-methyl transferase (COMT) reducing inhibition of active transport of Levodopa (by metabolite 3-O-methyldopa)
Mechanisms of DOPA and Metabolism Modifiers in Parkinson Disease Waters, C.H. Advances in Managing Parkinson’s Disease, Hospital Practice 06 (2001): http://www.hosppract.com/issues/2001/06/waters.htm.